|
|
|
|
|
Breast Metastasis as Initial Presentation of Silent, Synchronic, Widely Metastatic Renal Cell Carcinoma
|
|
|
Laisa Socorro Briongos-Figuero1, Esther Giménez-Barriga1, Sara Plaza-Loma2, Fátima Castroviejo-Royo3, Germán Marcos-García4, Tomás Zamora-Martínez5, José Ignacio Blanco-Álvarez6
Departments of Internal Medicine1, Radiology2, Urology3, Oncology4, Pathology5 and General Surgery6; Rio Hortega University Hospital. C/Dulzaina 2, 47012 Valladolid, Spain. |
|
|
|
|
|
Corresponding Author:
|
Dr. Laisa Socorro Briongos-Figuero
Email: laisadoc@hotmail.com
|
|
|
|
|
|
|
|
|
Received:
03-SEP-2015 |
Accepted:
21-OCT-2015 |
Published Online:
20-NOV-2015 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Metastasis to breast from extra-mammary sites is much less common as compared to primary ones and only few cases are reported in the literature. Furthermore, very little is known about prognosis and treatment of patients with solid neoplasms metastatic to the breast. If a breast lump is found, it is recommended to perform a bilateral mammogram specially when there is a rapidly enlargement. Here, we describe a case of a young woman with synchronic breast metastasis from asymptomatic, widely spread, renal cell carcinoma, Furhman grade 4. RCC is one of the most aggressive urologic tumors and rarely metastasizes to the breast. This phenomenon takes place in less than 3% of all metastatic renal cell carcinoma and the appearance as first sign of renal disease is exceptional. This case illustrates the importance of histopathological investigation in a breast mass and the potential for rare sites of metastasis in order to prevent unnecessary radical procedures. Also, this report contributes to importance of a proper diagnosis when rare sites of metastatic deposit, like breast, are detected, especially if there is no previous history of neoplasm. |
|
|
|
|
|
Keywords :
|
Angiogenesis Inhibitors, Breast Neoplasms, Carcinoma, Renal Cell, Neoplasm.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff24e0090000004a04000001000700 6go6ckt5b5idvals|539 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Metastasis to the breast from extra-mammary tumors occurs rarely, but it must be considered in the differential diagnosis of a rapidly enlarging breast mass. Indeed, this entity is increasing as patients live longer with malignant diseases [ 1]. In the same way, renal cell carcinoma (RCC) rarely metastasizes to the breast and this phenomenon take place in less than 3% of all metastatic RCC [ 2, 3]. Despite its rarity and difficulties in obtaining a correct diagnosis, a high index of suspicion is necessary because treatment and prognosis differ when compared to primary breast cancer. We report here a case of a young woman with synchronic breast metastasis from asymptomatic renal cell carcinoma.
Case Report
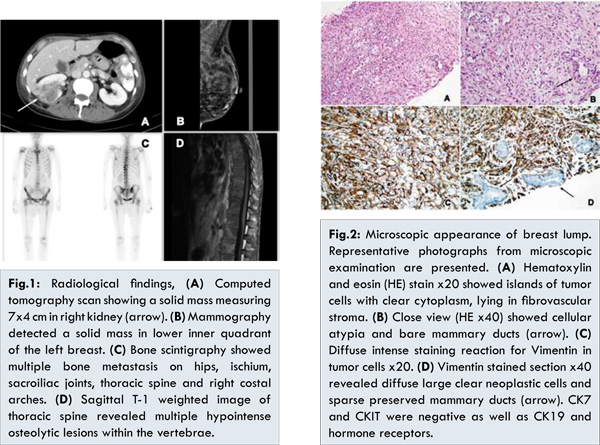
A 46-years-old woman without significant medical history presented with 5-week history of painless, mobile, rapidly growing breast mass. This was accompanied by lumbo-sciatalgia pain for past 3 weeks. No history of fever or weight loss was elicited. Laboratory test and spine X-ray revealed nothing remarkable. A tender, palpable, painless and mobile lump was detected in left breast with no skin infiltration. There was no clinically palpable cervical or axillary lymphadenopathy. Bilateral mammography confirmed a dense, multilobulated, solid, non-speculated mass measuring 12 mm in diameter, located in lower inner quadrant of left breast without micro-calcifications or adjacent parenchymal distortion [Fig.1B]. Histopathology of an ultrasound-guided tru-cut biopsy was consistent with metastatic deposit from renal cell carcinoma (RCC) by clear neoplastic cells that showed strong positivity in immunohistochemistry for Vimentin, CD10 and RCC marker while CK7, CKIT, CK19 and hormone receptors were negative as well as [Fig.2]. 99mTc tagged to HDP (hydroxymethylene diphosphonate) bone scintigraphy showed a solid mass measuring 7x4 cm in right kidney, multiple bilateral lung nodules and osteolytic lesions in axial skeleton (hips, ischium, sacroiliac joints, thoracic spine and costal arches) suggesting widespread vertebral metastatic disease [Fig.1A,C,D] Final diagnosis was silent RCC with synchronic breast, lung and bone metastasis.
Her case was discussed by a multidisciplinary teamwork and laparoscopic radical right nephrectomy was performed with no complication. Histopathological examination confirmed clear cell RCC, Furhman grade 4, stage pT3apN0pM1. After surgery, she was given 3 cycles of systemic tyrosine kinase inhibitor sunitinib therapy with good tolerance. Unfortunately, she suddenly developed severe dyspnea and fever due to bilateral pneumonia and expired.
Discussion
Renal cell carcinoma (RCC) is one of the most aggressive urologic tumors with unpredictable metastatic behavior. Vascular invasion is most common pathway of spread and 30% of patients have metastasis at the time of diagnosis, most commonly in lung (70%), lymph-nodes (55%), bone (42%), liver (41%), and central nervous system (11%) [ 3, 4].
Metastasis to the breast from extra-mammary tumors ranges 0.5% to 2%, usually due to melanoma, lymphoma or rhabdomyosarcoma in women and prostate cancer in men [ 1, 5]. Accurate diagnosis is important to prevent unnecessary radical procedures and to institute an appropriate systemic oncologic therapy. Metastasis from RCC in breast is extremely rare and only few cases have been reported in literature, most of them years after a previous nephrectomy [ 4, 6, 7]. Moreover, breast metastasis as first sign of renal disease, as occurs in our patient, is exceptional [ 2, 8]. To best of our knowledge, this is the first case of synchronic breast metastasis from RCC described from Spain. Clinically, breast metastasis presenting as painless, mobile mass, and skin dimpling is rare leading to delayed diagnosis [ 3, 9]. Axillary node involvement is uncommon. Mammogram shows well-circumscribed lesions that lack micro-calcifications mimicking benign lesion so awareness of breast secondaries is essential to get prompt diagnosis [ 2- 4]. The key for diagnosis is pathological investigation. Unfortunately, there is no curative treatment for disseminated RCC and prognosis is poor, but it is expected to increase survival in tyrosine kinase inhibitors era [ 3]. In our case, solitary breast metastasis was the first presentation of asymptomatic RCC and immunohistochemistry was very helpful to get diagnosis, avoiding an unnecessary mastectomy.
Conclusion
This case emphasizes the importance of a proper diagnosis when rare sites of metastatic deposit, like breast, are detected, especially if there is no previous history of neoplasm. Finally, a multidisciplinary strategy is needed to improve understanding of RCC presentation and management of breast metastasis.
References
- Vaughan A, Dietz J, Moley J, DeBenedetti M, Aft R, Gillanders W, et al. Metastatic disease to the breast: the Washington University experience. World Journal of Surgical Oncology. 2007;5:74.
- Alzaraa A, Vodovnik A, Montgomery H, Saeed M, Sharma N. Breast metastasis from a renal cell cancer. World J Surg Oncol. 2007;5:25.
- Falco G, Buggi F, Sanna PA, Dubini A, Folli S. Breast metastases from a Renal Cell Carcinoma. A case report and review of the literature. Int J Surg Case Rep. 2014;5:193-195.
- Mahrous M, Al Morsy W, Al-Hujaily A, Al-Sulimani S. Breast metastasis from renal cell carcinoma: rare initial presentation of disease recurrence after 5 years. J Breast Cancer. 2012;15:244-247.
- Williams SA, Ehlers RA, Hunt KK, Yi M, Kuerer HM, Singletary SE, et al. Metastases to the breast from nonbreast solid neoplasms. Cancer. 2007;110:731-737.
- Ganapathi S, Evans G, Hargest R. Bilateral breast metastases of a renal carcinoma: a case report and review of the literature. BMJ Case Reports. 2008;2008.
- Bortnik S, Cohen DJ, Leider-Trejo L, Ron IG. Breast metastasis from a renal cell carcinoma. Isr Med Assoc J. 2008;10:736-737.
- McLauglin SA, Thiel DD, Smith SL, Wehle MJ, Menke DM. Solitary breast mass as initial presentation of clinically silent metastatic renal cell carcinoma. Breast. 2006;15:427-429.
- Solaini L, Bianchi A, Filippini L, Lucini L, Simoncini E, Ragni F. A Mammary Nodule Mimicking Breast Cancer. International Surgery. 2014;99:200-202.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Briongos-Figuero LS, Giménez-Barriga E, Plaza-Loma S, Castroviejo-Royo F, Marcos-García G, Zamora-Martínez T, Blanco-Álvarez JIBreast Metastasis as Initial Presentation of Silent, Synchronic, Widely Metastatic Renal Cell Carcinoma.JCR 2015;5:499-502 |
|
Briongos-Figuero LS, Giménez-Barriga E, Plaza-Loma S, Castroviejo-Royo F, Marcos-García G, Zamora-Martínez T, Blanco-Álvarez JIBreast Metastasis as Initial Presentation of Silent, Synchronic, Widely Metastatic Renal Cell Carcinoma.JCR [serial online] 2015[cited 2026 Jun 6];5:499-502. Available from: https://www.casereports.in/articles/5/2/Breast-Metastasis-as-Initial-Presentation-of-Silent-Synchronic-Widely-Metastatic-Renal-Cell-Carcinoma.html |

|
|
|
|
|