Introduction
Carcinosarcoma/metaplastic breast carcinoma (MBC) is a rare and heterogeneous group of malignancies that constitutes less than 1% of all breast cancers [
1]. These neoplasms are characterized by adenocarcinoma with dominant areas of spindle cells, squamous and/or other mesenchymal differentiation [
2-
5]. Nodal involvement has been shown to be less common compared to typical breast adenocarcinomas, with an incidence ranging from 6%-26%. Most metaplastic cancers are estrogen receptor (ER), progesterone receptor (PR) and Her2-neu negative [
6]. The major criterion for a diagnosis of metaplastic carcinomas of the breast is the presence of overt carcinomas that are composed largely of squamous and spindle cells, and those with a sarcoma-like growth pattern including heterogeneous elements such as bone and cartilage [
7]. Oberman separated metaplastic carcinomas into three groups: spindle cell carcinoma, invasive ductal carcinoma with extensive squamous metaplasia, and invasive carcinoma with pseudosarcomatous metaplasia. However, he suggested that these tumors were variants of a single entity because of the lack of correlation of microscopic pattern with prognosis, as well as the apparent overlapping microscopic findings [
1]. Pitts et al. [
8] recommended that sub-classification of metaplastic carcinomas was of greater pathologic than clinical interest. In contrast, some investigators have reported that different pathologic patterns may have prognostic significance, and prognosis is particularly poor for those with carcinosarcoma. In an attempt to better understand the characteristics of the entity, we present a rare case of a 43-year old woman presenting with a large breast mass.
Case Report
A 43-year old perimenopausal woman was admitted with a large right breast mass which measured 15x10 cm. The patient stated that the mass began as a very small bump that she ignored until it started to grow over the next 6 months and cause pain and started interfering with daily work. She had no history of trauma, nipple discharge, or other previous breast diseases. Her primary physician referred her to a surgeon who performed excision of the mass without pre-operative radiodiagnostics.
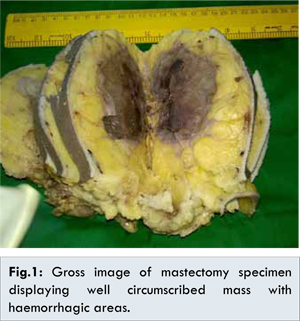
The patient had no event after surgery till 2 months when a small nodule started to arise again from the site of excision. On physical examination, a diffuse mass was palpated of about 15 cm in largest dimensions which involved almost all the quadrants of right breast. No axillary, infraclavicular, supraclavicular or cervical lymph nodes were palpated as such. Ultrasonography of the right breast revealed a radiopaque lesion of size 15x10x7 cm with well delineated mass densities and focal microcalcifications. The patient was given options of fine needle aspiration cytology and biopsy for the screening of the nature of the lesion before performing radical mastectomy. She denied and opted for radical mastectomy. This encompassed removal of the entire pectoralis major and minor musculature down to the right chest wall, and a complete level III axillary lymph node dissection was performed. The skin flaps were viable, not grossly involved with tumor, and were able to be closed primarily. Gross examination of the specimen [Fig.1] revealed a well circumscribed mahogany brown solid tumor. The tumor measured 15x10 cm in length and width, and 5.0 cm in height with the solid part measured 4.0?×?4.0?×?3.5 cm. Dark-red intracystic hemorrhage was noted.
Microscopically [Fig.2] the tumor exhibited a biphasic pattern consisting of epithelial and mesenchymal components. Intraductal cell masses were formed in the epithelial components with obvious heteromorphism and central necrosis. Meanwhile, a large number of spindle cells with some multinucleate giant cells were present in the mesenchymal components in an interlaced pattern. No metastasis was found in lymph nodes. Immunohistochemical profile [Fig.3] revealed a neoplasm with a dimorphic histology. The epithelial (carcinomatous) component stained positive for pan-cytokeratin immunostain and the mesenchymal (sarcomatous) component was negative for CAM5.2, actin and desmin, but positive for Vimentin. The tumor was estrogen and progesterone receptor negative. Pathological diagnosis of mixed epithelial and mesenchymal metaplastic carcinoma (carcinosarcoma) was made on the basis of the above mentioned findings of histopathology and immunohistochemistry.
Discussion
Carcinosarcoma of the breast is a malignant sarcomatoid metaplasia of epithelial carcinoma and is rare. It is an aggressive tumor constituting less than 1% of all breast cancers. It accounts for 0.08% - 0.2% of all malignant breast lesions. Wargotz and Norris suggested that carcinosarcoma of the breast, in which an epithelial-mesenchymal transition zone does not exist, should be distinguished from other MBC diseases. Such diagnosis is not difficult with detailed histological investigation. Grossly, it tends to be well circumscribed as shown in Fig.1. Histologically, it is a poorly differentiated heterogeneous tumor containing ductal carcinoma cells admixed with areas of spindle, squamous, chondroid, or osseous elements. Classification of metaplastic carcinoma was proposed by the World Health Organization in 2003 as i) squamous cell carcinoma, ii) adenocarcinoma with spindle cell proliferation, iii) adenosquamous, including mucoepidermoid, and iv) mixed epithelial and mesenchymal. Subtypes of mixed epithelial and mesenchymal carcinoma includes a) carcinoma with chondroid metaplasia, b) carcinoma with osseous metaplasia, and c) carcinosarcoma [
9].
Carcinosarcoma is a general term describing biphasic lesions that simultaneously contain malignant epithelial and malignant mesenchymal tissue components and distinct positive reactions are displayed in immunohistochemical examination [
10]. The origin of breast carcinosarcoma is far from clear. They have been reported to develop from existing cystosarcoma phyllodes, fibroadenoma and cystic backgrounds [
11]. Carcinosarcoma is characterized by the loss of intercellular adhesion, down-regulation of epithelial makers (cytokeratins), upregulation of mesenchymal markers [Vimentin and smooth muscle actin (SMA)], increase in motility, invasiveness, and metastatic capabilities [
12-
13]. In the present case, immunohistochemical staining showed the epithelial component to be positive for cytokeratin, while sarcomatous cells were positive for smooth muscle actin, and both components were positive for Vimentin. Therefore, the possibility of the tumor being derived from a cell with potential biphasic differentiation was considered.
Carcinosarcoma of the breast should be distinguished from metaplastic carcinoma, including spindle cell carcinoma, carcinoma with cartilaginous or osseous metaplasia, matrix producing carcinoma, fibrosarcoma and other types of sarcoma. The most important finding to differentiate metaplastic carcinoma from carcinosarcoma is whether a transition zone exists. Carcinoma of the breast can undergo spindle-cell and other metaplasia, such as fibroblastic, chondroid, osseous, or osteoblastic. Although these metaplastic and infiltrative cancer cells form pseudosarcomatous stroma, as if carcinomatous components are admixed with sarcomatous components, a transition zone is always seen between these two components. The cumulative 5-year survival rate of carcinosarcoma is 49%. The survival rate for spindle cell carcinoma and matrix-producing carcinoma is 64% and 68%, respectively, so these tumors should be distinguishable other than by the difference in their prognosis [
14]. Though any type of sarcoma arising from mesenchymal tissue can be confused with carcinosarcoma, there is no proof of malignant epithelial elements in these sarcomas. A carcinomatous component may be very minor in carcinosarcoma; therefore, carcinomatous elements can be lost by inadequate sampling and diagnosed as sarcomas, making careful study necessary to corroborate the diagnosis [
15].
Although relatively rare and histologically heterogeneous, their clinical manifestations are often similar. They are often palpable, mobile, and large, showing benign imaging features such as a round or oval shape with circumscribed margins. Meanwhile, estrogen, progesterone, and Her-2 are less frequently shown to be positive, with lower rates of axillary node involvement. Carcinosarcoma should be differentiated from other metaplastic carcinomas. The most important evidence is the non-existent region of transition between the 2 elements. Thus, a thorough pathological search for the transitional area is paramount. Carcinosarcoma can also presents as malignant phyllodes tumor accompanied by malignant epithelial components which may constitute only a small proportion of the entire carcinosarcoma [
16].
Conclusion
In summary, carcinosarcomas should be included in the differential diagnosis of breast cancers. Estrogen and progesterone receptors are negative in the majority of metaplastic carcinomas of the breast. The patient in this case presented with longer duration of symptoms, higher grade, larger tumor size, thus having a less favourable prognosis.
References
- Oberman HA. Metaplastic carcinoma of the breast. A clinicopathologic study of 29 patients. Am J Surg Pathol. 1987;11:918-929.
- Rauf, F, Kiyani, N, Bhurgri, Y. Metaplastic Carcinoma of Breast, an Intriguing Rarity. Asian Pacific Journal of Cancer Prevention. 2006;7:667-671.
- Pitts WC, Rajos VA, Gaffey MJ, Rouse RV, Esteban J, Frierson HF, et al. Carcinomas with Metaplasia and Sarcomas of the Breast. American Journal of Clinical Pathology. 1991;95:623-632.
- Tavassoli FA. Classification of Metaplstic Carcinomas of the Breast. Annual Review of Pathology. 1992;27:89-119.
- Rosen PP. Rosen’s Breast Pathology. Lippencott-Raven Philadelphia: 1997;375-395.
- Wargotz ES, Norris HJ. Metaplastic carcinomas of the breast: III. Carcinosarcoma. Cancer. 1989;64:1490-1499.
- Kaufman MW, Marti JR, Gallager HS, Hoehn JL. Carcinoma of the breast with pseudosarcomatous metaplasia. Cancer. 1984;53:1908-1917.
- Pitts WC, Rojas VA, Gaffey MJ, Rouse RV, Estaban J, Frierson HF, et al. Carcinomas with metaplasia and sarcomas of the breast. Am J Clin Pathol. 1991;95:623-632
- Harris M, Persaud V. Carcionsarcoma of the breast. J Pathol. 1974;112:99-105.
- Tavassoli FA, Devilee P. Pathology and Genetics of Tumours of the Breast and Female Genital Organs. Volume 4. Lyon, France: IARC Press; 2003. (World Health Organization Classification of Tumours).
- Bolton B, Sieunarine K. Carcinosarcoma: a rare tumour of the breast. Aust NZ J Surg. 1990;60:917-919.
- Gurleyik E, Yildirim U, Gunal O, Pehlivan M. Malignant Mesenchymal Tumor of the Breast: Primary Chondrosarcoma. Breast Care. 2009;4:101-103.
- Thiery JP. Epithelial-mesenchymal transitions in tumour progression. Nat Rev Cancer. 2002;2:442-454.
- Thompson EW, Newgreen DF, Tarin D. Carcinoma invasion and metastasis: a role for epithelial-mesenchymal transition? Cancer Res. 2005;65:5991-5995.
- Smitt MC. Metaplastic breast cancer. Clin Breast Cancer. 2003;4:210-211.
- Azzopardi JG. Problems in breast pathology. WB Saunders, Philadelphia: 1979, pp.373-378.