Introduction
Teratoma is a tumor originating from totipotent germ cells [
1]. Mature teratomas are the most common germ cell tumors [
1,
2]. Germ cell tumors are predominantly found in the gonads and the most common extra-gonadal site is the anterior mediastinum [
2]. Intrapulmonary location in the mediastinum is very rare [
2]. A total of 67 cases have been reported in literature upto 2007, since its first report in 1839 [
3]. Till date, very few cases of intrapulmonary teratoma has been reported from India [
4]. This case of benign cystic lung lesion was provisionally diagnosed and even operated with the diagnosis of hydatid cyst in mind but later turned out to be a teratoma on gross and microscopic examination.
Case Report
A 28 year old female patient presented with recurrent episodes of left sided dull aching chest pain for last one month, along with dry cough for last 7 days. Shortness of breath was associated with the chest pain. No history of fever, weight loss or haemoptysis was reported. No previous history of any shortness of breath or any allergy was present.
On clinical examination, vitals were stable, patient was afebrile, oxygen saturation 94%, respiratory rate was 16/min but respiratory movement was slightly decreased on the left side. On auscultation, decreased vesicular breath sounds were noted in the left side. Rest of the systemic examinations was within normal limits.
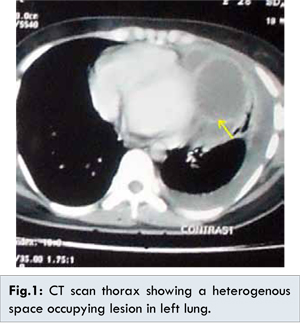
Chest X-ray revealed a left sided large cystic opacity. No air fluid level was detected. CT scan thorax showed a well-defined space occupying lesion measuring 16.7x11.2x9.6 cm with pleural effusion and collapse. The lesion showed heterogenous density containing soft tissue elements, cystic areas and foci of calcifications. Perilesional inflammatory change and thickening was noted. No mediastinal lymphadenopathy was seen [Fig.1]. Broncho-alveolar lavage fluid examination showed scanty mature squamous cells and cluster of bronchoepithelial cells without any evidence of dysplasia. Fibreoptic bronchoscopy under local anaesthesia revealed external compression at the level of left intermediate bronchus. No intrabronchial mass or inflamed area was noticed. Pulmonary function test showed decreased FVC and 25%-75% PEF indicating small airway obstruction.
Enucleation of the tumor by left anterolateral thoracotomy was performed and the cyst was identified in the upper lobe of left lung. Content was aspirated using a 20 mL syringe and the tumor was debulked in pieces along with surrounding compressed lung tissue [Fig.2]. The tissue sent for histopathological examination was in the form of grayish brown irregular pieces. It contained yellowish and whitish areas, altogether measuring 7x4x2 cms. On microscopic examination, sections showed stratified squamous epithelium along with adnexal components, adipose tissue, cartilage, calcified osteoid, and few undifferentiated glands. Histopathological diagnosis of mature cystic teratoma was given [Fig.3,4]. Post-operative recovery was uneventful and patient is in close follow up.
Discussion
Mature teratomas are the most common germ cell tumors followed by seminoma [
2]. It comprises recognizable mature or immature cells or tissue belonging to one or more than one germ cell layer (sometimes all three) [
1]. Various theories have been postulated about their origin. One theory suggest that they arise from the displaced thymic tissue of 3rd pharyngeal pouch [
3]. Another study claims that the origin of intrapulmonary cystic teratomas are from aberrant thymic tissue [
3]. Yet in another study it has been proposed that primordial teratoma focus in the mediastinum is caught up by the respiratory outgrowth resulting in their intrapulmonary location [
4]. However, intrapulmonary teratomas are very rare and only a few cases have been reported since its first description given by Mohr in 1839 [
2-
4].
Pulmonary teratomas are commonly reported in the 2nd to 4th decade of life with slight female preponderance. Clinically the most common presentation is chest pain followed by cough and haemoptysis [
4]. Trichoptysis is the most specific symptom but not seen in our case [
3]. Most common location is in the upper lobes of the lung as in our case [
4,
5].
Radiologically it may appear as a cavitary lesion, consolidation or as a heterogenous space occupying lesion as seen in this case containing various elements like fat, fluid and foci of calcification [
3]. Since intrapulmonary teratoma is a rare tumor, initially a provisional diagnosis of hydatid cyst was made in our case. Later on after doing CT scan and excision of the tumor followed by histopathological examination the diagnosis was confirmed.
Histologically components of all three germ layers were recognised. Ectodermal component identified were skin and adenxal glands. Mesodermal component like adipose tissue and cartilage and bone were seen. Endodermal component identified were glandular elements.
Surgical resection is the treatment of choice. In our case, thoracotomy was performed followed by aspiration of the content and debulking of the tumor in pieces. The surrounding lung tissue was fibrosed and consolidated. After the operation the patient improved and the remaining lung tissue reverted back to normal as seen in the post-operative CT scan.
Conclusion
Teratomas are the commonest germ cell tumors but its location inside lung makes this case an unusual one. Possibility of teratomas should be kept as one of the differential diagnosis when we consider cystic lung lesions.
References
- Kumar V, Abbas AK, Aster JC, editors. Robbins and Cotran .Pathologic basis of disease. 9th edition. Philadelphia: Saunders; 2015. Vol 2. 1012-1021
- Ahmad Dar R, Mushtaque M, Hamid Wani S, Malik R. A Giant Intrapulmonary Teratoma: A Rare Case. Case Reports in Pulmonology. Volume 2011 (2011), Article ID 298653.
- Vigg A, Khulbey SK, Agarwal SK, Dikshit V, Sathpathy A, Srinivas U, Swarnalata G, Modi T, Hemalatha AS. Intra-pulmonary Teratoma: A Rare Case. Indian J Chest Dis Allied Sci. 2012;55:155-157.
- Sawant A, Gill N, Balasubramanian V. A Rare Case of Intrapulmonary Cystic Teratoma Mimicking Malignant Pulmonary Neoplasm. Chest. 2011;140 (4_MeetingAbstracts):3A.
- Saini ML, Krishnamurthy S, Kumar RV. Intrapulmonary mature Teratoma. Diagn Pathol. 2006;1:38.