Introduction
Amoebic liver abscess is the most common inflammatory space occupying lesion of liver with high mortality and morbidity [
1]. It is the third most common parasitic infestation in world having increased incidence in tropical countries [
2]. Amoebic liver abscess has highly variable presentation having diagnostic difficulty. Rupture into peritoneal and pleural cavity are common complications but rupture into abdominal wall and presenting as a tender inguinoscrotal swelling with acute abdomen is very rare. We report an extremely rare case of acute abdomen along with tender inguinoscrotal swelling following ruptured amoebic liver abscess.
Case Report
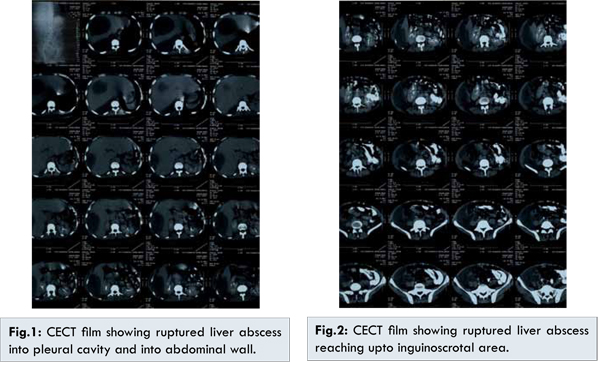
A 32 year old male was brought to surgical emergency department with complaints of pain in the right upper abdomen for one month, respiratory difficulty and swelling in right inguinoscrotal region for three days. He also had history of intermittent fever and cough with expectoration. On general physical examination patient was afebrile, dehydrated with pulse rate of 96/minute, blood pressure of 92/60 mm Hg and respiratory rate of 28/min. On abdominal examination, there was tenderness and guarding present over right hypochondrium, lumbar and right inguinoscrotal region along with a tender inguinoscrotal swelling of size 6x3 cm with inflamed overlying skin. Swelling was fluctuant but transillumination was negative. Systemic examination revealed significantly decreased air entry on right side of chest. The laboratory studies revealed haemoglobin 6.5 gm/dL and total leukocyte count of 18000/mm3 with increased polymorphs. Liver function test showed serum bilirubin was 2.5 mg/dL with mildly raised SGOT/PT and renal functions were normal. On chest X-ray, there was pleural effusion on right side. Ultrasonography revealed two hypoechoic lesions of size 10.7x10 cm and 10x7.7 cm in right lobe communicating with peritoneal cavity with right side pleural effusion. Chest drain was put on right side and 500 cc anchovy sauce pus was drained which was sent for microscopic examination and culture sensitivity of pus. Contrast enhanced computed tomography of abdomen was done which showed ruptured liver abscess into parieties and pus tracking along abdominal wall to inguinoscrotal region [Fig.1,2].
The first abscess was drained by right intercostal drainage while the second one was drained by an inguinal incision and putting a negative drain in the inguinal area, which drained the abscess from parieties as well as scrotal area. He was given intravenous antibiotics in form of ceftriaxone and high dose metrogyl. Patient started improving with the treatment, abscess sizes were reduced on subsequent ultrasounds, right lung expanded and chest tube was removed. The inguinal drain was removed after 21 days and patient was discharged in a stable condition from the ward.
Discussion
Amoebiasis has a worldwide distribution and is more common in tropical countries with areas having poor sanitation. Fortunately, hepatic liver abscess occurs only in 3%-7% of all patients with intestinal amoebiasis [
1]. Amoebic liver abscesses are more commonly located in right liver lobe [
2]. The abscess cavity can vary in size from 1-25 cms and if the condition remains untreated, it can rupture into adjacent organs/cavities.
The reported incidence of complications of amoebic liver abscesses vary from 20%-35% in earlier and 12%-20% in more recent series [
3]. Most common complications are related to rupture of the abscess into an organ or adjacent space. Common complications are those involving lung and pleura leading to empyema or pneumonitis and rupture of abscess into peritoneum leading to generalised or localised peritonitis [
4]. Apart from these relatively common complications, rare complications include rupture of the abscess into stomach, intestines and pericardium [
5].
Ultrasound abdomen is the investigation of choice for an uncomplicated liver abscess, but for complicated abscesses, CECT abdomen should be carried out before any intervention is made. CECT was diagnostic in the present case where patient was having two large abscesses, one of which was communicating with pleural cavity while the other had ruptured into the abdominal wall reaching upto inguinoscrotal area. Since we could locate the exact sites of perforations, the patient was managed only by intercostal drainage and incision and drainage of inguinal abscess. We could safely defer the exploratory laparotomy and the morbidities associated with it despite presence of abdominal signs.
Conclusion
The patient is being reported to highlight inguinoscrotal swelling with acute abdomen is very rare presentation of amoebic liver abscess. CECT abdomen is the investigation of choice in such cases which can diagnose the exact site of rupture of abscess. If the exact diagnosis is made preoperatively, they can be managed by local intervention only avoiding formal laparotomy.
References
- Sehgal D, Bhattacharya A, Bhattacharya S. Pathogenesis of infection of Entamoeba histolytica. J Biosci. 1996;21:423-432.
- Stanley SL Jr. Amoebiasis. Lancet. 2003;361:1025-1034.
- Mukhopadhyay M, Saha AK, Sarkar A, Mukherjee S. Amoebic liver abscess: presentation and complications. Indian J Surg. 2010;72:37-41.
- Maltz G, Knauer CM. Amoebic liver abscess: a 15 year experience. Am J Gastroenterol. 1991;86:704-710.
- Meng XY, Wu JX. Perforated amoebic liver abscess: clinical analysis of 110 cases. South Med J. 1994;87:985-990.