|
|
|
|
|
Invasive Mucinous Carcinoma Arising in a Background of Breast Fibroadenoma
|
|
|
benadryl pregnancy safety benadryl pregnancy dosage
Department of Anatomic and Molecular Pathology, College of Medicine, University of Lagos/ Lagos University Teaching Hospital, Idi-Araba, Lagos, Nigeria. |
|
|
|
|
|
Corresponding Author:
|
Dr. Anunobi CC
Email: dozieanunobi@yahoo.com
|
|
|
|
|
|
|
|
|
Received:
20-FEB-2015 |
Accepted:
26-JUN-2015 |
Published Online:
20-JUL-2015 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Mucinous carcinoma arising in a background of fibroadenoma is rare. We report a case of a 34 year old woman who presented in our hospital with a mobile mass in the right breast. Physical examination, breast ultrasound and fine needle aspiration cytology (FNAC) were all concordant for diagnosis of fibroadenoma. However microscopic examination of excisional biopsy revealed mucinous carcinoma within a background of fibroadenoma. The patient underwent right mastectomy with dissection of the right axillary lymph nodes. Nodal metastasis was not seen. She was also treated with chemotherapy and radiotherapy and has shown no sign of recurrence for more than one year since after surgery. This report highlights one of the pitfalls of FNAC, particularly in the diagnosis of mixed lesions of the breast. |
|
|
|
|
|
Keywords :
|
Breast Neoplasms, Mucinous Adenocarcinoma, Fibroadenoma, Mastectomy, Biopsy.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff049e070000000202000001001200 6go6ckt5b5idvals|489 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Fibroadenoma is a very common benign breast lesion typically occurring in patients between the ages of 20 and 35 years with incidence decreasing after 40 years. It is the commonest female benign breast tumor and usually single but in about a quarter of the cases they present as multiple tumors in the breast [1]. Malignant neoplasms arising in the background of fibroadenoma are rare. The most frequent types are lobular and ductal carcinoma in situ. Very few reported cases of mucinous carcinoma arising within a background of fibroadenoma are seen in literature [2]. To the best of our knowledge after an online search, this is the first of such case to be reported from Nigeria.
Case Report
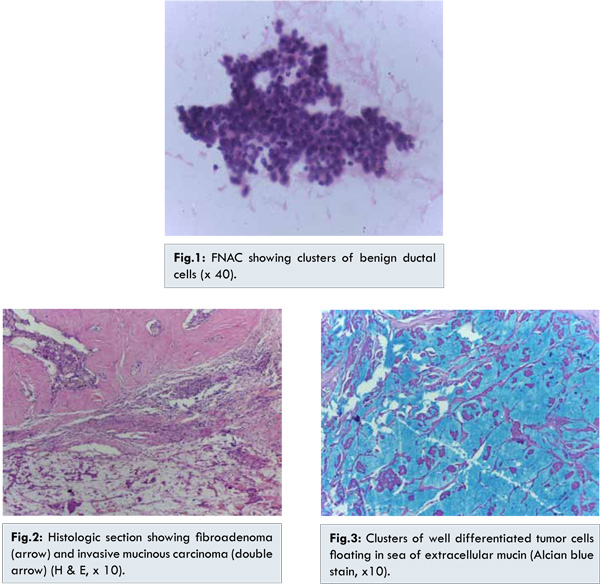
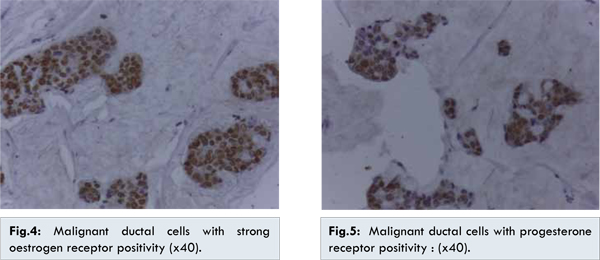
The patient is a 34-year old lady who presented to the clinician with a two month history of right breast lump. Clinical examination showed a well-defined and freely mobile breast lump in the upper outer quadrant of right breast measuring about 6x4 cm. There were no palpable axillary lymph nodes. Breast ultrasound scan showed an ellipsoid-shaped, hypoechoic mass with a regular outline measuring 5x3x2 cm. No calcification and no posterior acoustic shadowing or enhancement was seen. No area of hypervascularity was seen on Color Doppler. The conclusion was fibroadenoma of right breast and FNAC was advised by the radiologist. FNAC showed cohesive clusters of regular ductal epithelial cells with smooth nuclear borders, fine chromatin pattern and myoepithelial cells [Fig.1]. It was therefore reported as a benign lesion. A lumpectomy was done based on concordant diagnosis of fibroadenoma by clinical examination, ultrasound and FNAC. Gross appearance of the lump showed a firm encapsulated grayish white tissue measuring 5x2.5x2.0 cm. Cut section showed a firm grayish white surface with areas of gelatinous consistency. Microscopic examination showed pools of mucin containing islands and trabeculae of malignant epithelial cells. No evidence of carcinomatous emboli or perineural invasion was seen. However, the resection margins were not free of the tumor cells. Elsewhere were seen proliferating ducts compressed into slit-like spaces by the surrounding fibrocollagenous stroma. It was reported as mucinous carcinoma within a background of fibroadenoma [Fig.2]. Alcian blue stain demonstrated mucin lakes with floating tumor cells [Fig.3]. Immunohistochemistry studies showed positivity for oestrogen receptors (ER) and progesterone receptors (PR) [Fig.4,5]. The tumor cells were however negative for HER2 neu.
The patient was taken back to the theatre for right mastectectomy with axillary clearance. The lymph nodes were free of the tumor cells. She was given chemotherapy and radiotherapy and has shown no sign of recurrence for more than I year since after the last surgery.
Discussion
Carcinoma arising in a background of fibroadenoma was first described in 1931 by Cheatle and Cutler [3]. This uncommon phenomenon is found in 0.1% of cases and usually involves the epithelial component with large majority being in-situ [1]. Most often it is an incidental finding while examining biopsied specimens [1]. This rare case is reported here to highlight the need for core needle biopsy of large breast masses clinically diagnosed as fibroadenoma and also to emphasize the importance of histopathological evaluation of all breast masses irrespective of their clinical characteristics as benign lesions [4].
Malignant transformation in a fibroadenoma is a rare occurrence and peaks after many years of the peak incidence of fibroadenoma [2]. The two previously reported cases of mucinous carcinoma in a context of fibroadenoma occurred in patients older than 30 years [2,5]. This patient is aged 34 years and the tumor measured 5x2.5x2.0 cm. The dimensions of all fibroadenomata in the reported cases including this present one were greater than 2.5 cm. This case report with previous ones highlights the possibility of malignancy in a breast mass of greater than 2.5 cm in diameter in patients aged 30 years and above that will warrant surgical removal.
It is interesting to note that radiological (mammography) diagnosis in one of the two earlier reported cases was similar to this current case which diagnosed fibroadenoma [2]. The typical radiological findings of indistinct tumor borders and microcalcifications of breast malignant tumors were not seen in these cases. The classical smears of mucinous carcinoma of the breast are cellular, consisting of monomorphic cells with eccentric nuclei and whispy eosinophilic microvesicula cytoplasm in a background of copious extracellular mucin [6]. The mucin can be highlighted by PAS, Giemsa or Alcian blue stains. Fibroblasts and branching thin wall blood vessels are usually seen in the mucin [7]. Karyna et al. reported the presence of these thin walled capillaries in 96% of the breast colloid cancer cases they studied while also stating that colloid cancer generally lacks oval bare nuclei [8]. The aspirates in fibroadenoma are commonly very cellular and classically show stromal fragments, cohesive ductal cells exhibiting honeycomb appearance and myo-epithelial cells are seen as naked nuclei in the background. The breast aspirate features seen in the index case were in conformity with those of fibroadenoma.
Despite all the known features of mucinous carcinoma it may clinically and cytologically mimic myxoid fibroadenoma but close observation may show differences in arrangement of cells and absence of myoepithelial cells in mucinous carcinoma. Histologic examination is the gold standard for tissue diagnosis. Routine haematoxylin & eosin, Alcian blue stain and immunohistochemistry were used in the two earlier reports [2,5]. ER, PR and Her2 were all negative in Monsefi et al report [2]. Routine haematoxylin and eosin stain, Alcian blue stain and immunohistochemistry studies were all used in making the diagnosis of mucinous carcinoma within a background of fibroadenoma in this patient. The tumor cells expressed positive ER and PR staining but were however negative for HER2. This agrees with a study by Lacroix-triki et al. who reported that mucinous carcinomas always express ER (100%), but lack HER2 expression (97.71%) [9].
A carcinoma is assumed to arise within a fibroadenoma if the malignant cells are restricted to the fibroadenoma or show focal extension into the adjacent stroma or ducts [11]. According to Azzopardi, three possibilities exist for carcinoma arising from fibroadenoma [11]. An adjacent carcinoma that involves a fibroadenoma, a simultaneous cancer that involves the fibroadenoma as well as adjacent breast tissue or the carcinoma is entirely limited to fibroadenoma [11]. In this case, the adjacent carcinoma involves the fibroadenoma. Dupont et al. in a retrospective cohort study of 1835 patients with fibroadenoma diagnosed between 1950 and 1968 in the USA reported that fibroadenoma is a long-term risk factor for breast cancer [12]. Complex fibroadenomas, proliferative breast disease, or a family history of breast cancer have all been reported to increase the risk for female breast cancers [12]. This patient does not have positive family history and the fibroadenoma was not the complex type. She was not evaluated for BRCA gene mutation.
Sarela et al. had earlier advised that since there are no established clear cut clinical criteria to suggest malignant transformation in a fibroadenoma; histopathological examination would be required to establish definitive diagnosis [13]. Signs of malignant transformation in a fibroadenoma may also not be radiologically evident as demonstrated in this case [14]. This patient had right mastectomy, axillary clearance with radiotherapy and chemotherapy and has shown no sign of recurrence for more than one year since after surgery. The axillary nodes were free of malignant cells.
Even though FNAC of a breast lump is an accepted and established laboratory method of determining the nature of a breast lump with sensitivity and specificity of 96.42% and 100% respectively, it is not an alternative to histological diagnosis of breast lump especially in females older than 35 years [15].
Conclusion
This report highlights one of the pitfalls of FNAC, particularly in the diagnosis of mixed lesions of the breast. Core needle biopsy with histologic evaluation is advised for breast masses greater than 2.5 cm including those clinically and radiologically diagnosed as benign in patients aged 30 years and above.
References
- Rosai J. Rosai and Ackerman’s Surgical Pathology. 10th ed. Vol. 2. Edinburgh; New York: Mosby; 2011. pp.1668.
- Monsefi N, Nikpour H, Safavi M, Lashkarizadeh MR, Dabiri S. Mucinous subtype of invasive ductal carcinoma arising within a fibroadenoma. Arch Iran Med. 2013;16(6):366-368.
- Cheatle GL, Cutler M. Tumours of the breast: Their pathology, symptoms, diagnosis and treatment. London: Edward Arnoled & Co; 1931:483-484.
- Hemalatha AL, Raghupathi AR, Karthikeyan TM, Kumar DB, Shashidar HB. Carcinoma within a fibroadenoma: a case report. Indian J Pathol Microbiol. 2006;49(4):592-594.
- Charfi L, Mrad K, Sellami R, Driss M, Sassi S, et al. Invasive mucinous carcinoma arising within breast fibroadenoma. Pathologica. 2008;100(3):199-201.
- Shabb NS, Boulos FI, Abdul-Karim FW. Indeterminate and Erroneous Fine- Needle Aspirates of Breast with Focus on the “True Gray Zone”: A review. Acta Cytologica. 2013;57: 316-331.
- National Cancer Institute Fine- Needle Aspiration of Breast Workshop Subcommittees: The uniform approach to breast fine –needle aspiration biopsy. Diagn Cytopathol. 1997;16:295-311.
- Karyna Ventura, Joan Cangiallera, Irene Lee, Andre Moreira, Jerry Waisman, et al. Aspiration biopsy of mammary lesions with abundant extracellular mucinous material. Am J Clin Pathol. 2003;120:194-202.
- Lacroix-Triki M, Suarez PH, MacKay A, Lambros MB, Natrajan R, et al. Mucinous carcinoma is genomically distinct from invasive ductal carcinoma of no special type. J Pathol. 2010; 222(3):282-298.
- Pick PW, Iossifides IA. Occurrence of breast carcinoma within a fibroadenoma: a review. Arch Pathol Lab Med. 1984;108:590-596.
- Azzopardi JG, Ahmed, Mills RR: Problems in Breast Pathology. In: Benigton JC, ed. Major problems in pathology. Edinburgh: WB Saunders Company Ltd; 1979:325-328.
- Dupont WD, Page DL, Part FF, Vnencak-Jones CL, Plummer Jr WD, et al. Long-term risk of breast cancer in women with fibroadenoma. N Engl J Med. 1994;331(1):10-15.
- Sarela AI, Madvanur AA, Soonawala ZF, Shah HK, Pandit AA, et al. Carcinoma in a fibroadenoma. J Postgrad Med. 1995;41(1):19-20.
- Kuijper A, Preisler-Adams SS, Rahusen FD, Gille JJ, van der Wall E, et al. Multiple fibroadenomas harbouring carcinoma in situ in a woman with a family history of breast/ovarian cancer. J Clin Pathol. 2002; 55(10):795-797.
- Aslam S, Hameed S, Afzal T, Hussain A. Correlation of FNAC and histological diagnosis in the evaluation of breast lumps. JUMDC. 2012;3(2):1-7.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
CC Anunobi, AAF Banjo, TK AlawodeInvasive Mucinous Carcinoma Arising in a Background of Breast Fibroadenoma.JCR 2015;5:307-311 |
|
CC Anunobi, AAF Banjo, TK AlawodeInvasive Mucinous Carcinoma Arising in a Background of Breast Fibroadenoma.JCR [serial online] 2015[cited 2026 May 22];5:307-311. Available from: http://www.casereports.in/articles/5/2/Invasive-Mucinous-Carcinoma-Arising-in-a-Background-of-Breast-Fibroadenoma.html |

|
|
|
|
|