|
|
|
|
|
NPM1-mutated Acute Myeloid Leukemia Associated with Atypical Megakaryocytic Hyperplasia and Myelofibrosis Mimicking a Myeloproliferaive Neoplasm
|
|
|
|
T Sun, LJ Medeiros, C Bueso-Ramos
Department of Hematopathology, The University of Texas MD Anderson Cancer Center, Houston, TX USA. |
|
|
|
|
|
Corresponding Author:
|
|
Dr. Tsieh Sun
Email: tsun5@mdanderson.org
|
|
|
|
|
|
|
|
|
Received:
21-AUG-2015 |
Accepted:
16-SEP-2015 |
Published Online:
10-OCT-2015 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Nucleophosmin (NPM1) mutation is a frequent finding in acute myeloid leukemia (AML), occurring in 60% of adult cases with a normal karyotype [1]. Normally, NPM1 is located in the nucleus of myeloid cells, but NPM mutants are aberrantly localized to the cytoplasm of leukemic blasts, due to frameshift mutations involving one allele of the NPM1 gene [1,2,3]. NPM1-mutated AML is associated with unique gene expression profile and microRNA (miRNA) signatures [3]. A paradoxical phenomenon in NPM1-mutated AML is an increased number of megakaryocytes in the bone marrow associated with thrombocytopenia. A mouse model with NPM1 mutation also showed increased megakaryocytes with thrombocytopenia, but no evidence of leukemia [3]. A similar phenomenon was observed in human cases of NPM1 mutated AML [3]. Flow cytometric immunophenotypic analysis of the mouse model suggested that NPM1 mutant blocks megakaryocyte differentiation rather than causing an increase in the number of megakaryocytes secondary to platelet destruction [3]. However, no atypical megakaryocytic hyperplasia with myelofibrosis has been reported in NPM1-mutated AML. We herein report a case of NPM1-mutated AML with features mimicking primary myelofibrosis emerging in the remission period.
|
|
|
|
|
|
Keywords :
|
Blood Platelets, Frameshift Mutation, Acute Myeloid Leukemia, Megakaryocytes, Thrombocytopenia.
|
|
|
|
|
|
|
|
|
|
|
|
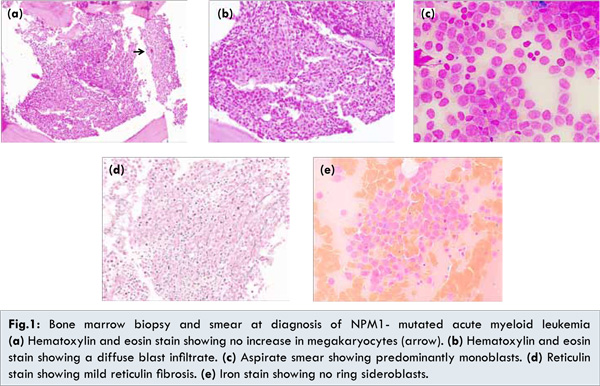
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffe443090000001604000001000400 6go6ckt5b5idvals|523 6go6ckt5b5|2000F757Tab_Articles|Fulltext A 69-year-old woman was found to have leukocytosis and circulating blasts in January, 2015. Further workup at another hospital 1 month later revealed AML with monocytic differentiation and 63% blasts [Fig.1a,b,c]. Mild reticulin fibrosis was observed [Fig.1d], but no morphologic evidence of dysplasia or myeloproliferative neoplasm was identified. Iron stain showed no ring sideroblasts [Fig.1e]. A peripheral blood smear revealed a total leukocyte count of 18.5 x 109/L, a hemoglobin level of 12.5 g/dL and a platelet count of 206 x 109/L.
The patient was treated with hydroxyurea and was referred to our hospital in March, 2015. At that time, physical examination showed no splenomegaly. Bone marrow aspiration and biopsy showed AML with 36% blasts and myelofibrosis (MF-2). A peripheral blood smear showed macrocytic anemia, thrombocytopenia (platelets 43 x 109/L) and a normal leukocyte count with 3% blasts. Conventional cytogenetic analysis showed a complex karyotype with trisomy 8 and del(20). PCR showed NPM1 mutation, but no FLT3 or CEBPA mutations. FISH analysis identified trisomy 8, but no BCR/ABL1, PML/RARA, MLL, CBFB or AML1/ETD.
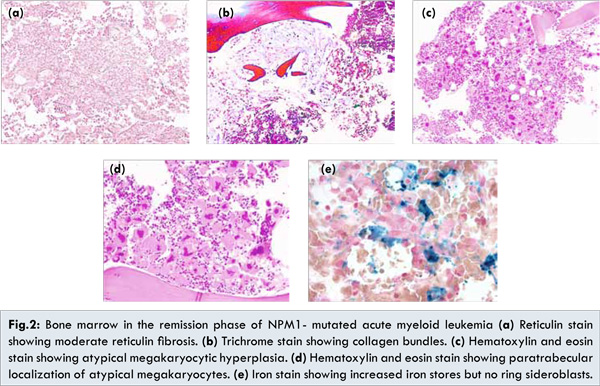
The patient was enrolled on a protocol consisting of decitabine in combination with vosaroxin. A repeat bone marrow aspiration and biopsy 3 weeks later showed no blasts, but myelofibrosis (MF-2) persisted [Fig.2a,b]. In addition, there was marked atypical megakaryocytic hyperplasia in an intertrabecular and paratrabecular distribution [Fig.2c,d]. No dysplastic changes and ring sideroblasts [Fig.2e] were identified. The platelet count was 55 x 109/L. PCR was negative for NPM1 mutation. Results for a panel of genes associated with myeloproliferative neoplasms including JAK2-V617F, MPL and CALR were negative. A repeat bone marrow aspiration and biopsy 6 weeks later (4 months after initial diagnosis) showed no evidence of atypical megakaryocytic hyperplasia and the platelet count was normal (412 x 109/L).
We believe this case is of interest because the morphologic features at the time of remission of AML with monocytic differentiation were associated with some features of primary myelofibrosis. However, molecular genetic investigation and follow-up studies indicated that this was a transient phenomenon with no evidence of a myeloproliferative neoplasm. Previous studies in animals and humans have shown that NPM1 may induce the paradoxical phenomenon of megakaryocytic hyperplasia with thrombocytopenia [ 3]. Therefore, it is most likely that the transient atypical megakaryocytic hyperplasia in the case described here was associated with NPM1 mutation.
The atypical megakaryocytic hyperplasia probably developed after the second biopsy and persisted when the third biopsy was obtained. At that time, the level of mutant NPM1 may have been low (<2.5%), below the molecular assay’s sensitivity of detection. Alternatively, fibrotic changes may persist for a variable time interval even after NPM1 is eliminated.
Another possibility is that the patient may have an underlying myeloproliferative neoplasm, which emerged after the acute leukemia had subsided. This possibility is unlikely because (i) the patient did not have a history of thrombocytosis or elevated hemoglobin/hematocrit, (ii) studies of JAK2-V617F, MPL, CALR and BCR/ABL1 were negative and (iii) atypical megakaryocytic hyperplasia disappeared spontaneously without specific treatment.
The lesson from this case is that a misdiagnosis of primary myelofibrosis could be made in a treated case of NPM1-mutated AML, particularly if the patient’s history is unknown. Myeloproliferative neoplasms have been reported preceding, but not following, NPM1-mutated AML [ 4, 5, 6]. However, these two entities are probably not related to each other [4,5].
References
- Falini B, Mecucci C, Tiacci E, Alcalay M, Rosati R, Pasqualucci L, et al. Cytoplasmic nucleophosmin in acute myelogenous leukemia with a normal karyotype. N Engl J Med. 2005;352:254-266.
- Cheng K, Grisendi S, Clohessy JG, Majid S, Bernardi R, Sportoletti P, et al. The leukemia-associated cytoplasmic nucleophosmin mutant is an oncogene with paradoxial functions: Arf inactivation and induction of cellular senescence. Oncogene. 2007;26:7391-7400.
- Sportoletti P, Varasano E, Rossi R, Bereshchenko O, Cecchini D, Gionfriddo I, et al. The human NPM1 mutation A perturbs megakaryopoiesis in a conditional mouse model. Blood. 2013;121:3447-3458.
- Pasqualucci L, Li S, Meloni G, Schnittger S, Gattenlohner S, Liso A, et al. NPM1-mutated acute myeloid leukaemia occurring in JAK2-V617F+ primary myelofibrosis: de-novo origin? Leukemia. 2008;22:1459-1463.
- Roug AS, Nyvold CG, Juhl-Christensen C, Christensen M, Schnittger S, Hokland P. A patient with a 20-year lag phase between JAK2-V617F+ myeloproliferation and NPM1-mutated AML arguing against a common origin of disease. Eur J Haematol. 2011;87:461-463.
- Schnittger S, Bacher U, Haferlach C, Alpermann T, Dicker F, Sundemann J, et al. Characterization of NPM1-mutated AML with a history of myelodyplastic syndromes or myeloproliferative neoplasms. Leukemia. 2001;25:615-621.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Sun T, Medeiros LJ, Bueso-Ramos CNPM1-mutated Acute Myeloid Leukemia Associated with Atypical Megakaryocytic Hyperplasia and Myelofibrosis Mimicking a Myeloproliferaive Neoplasm.JCR 2015;5:434-437 |
|
Sun T, Medeiros LJ, Bueso-Ramos CNPM1-mutated Acute Myeloid Leukemia Associated with Atypical Megakaryocytic Hyperplasia and Myelofibrosis Mimicking a Myeloproliferaive Neoplasm.JCR [serial online] 2015[cited 2026 May 21];5:434-437. Available from: http://www.casereports.in/articles/5/2/NPM1-mutated-Acute-Myeloid-Leukemia-Associated-with-Atypical-Megakaryocytic-Hyperplasia-and-Myelofibrosis-Mimicking-a-Myeloproliferaive-Neoplasm.html |

|
|
|
|
|