Introduction
Complete diaphragmatic dome agenesis is the largest diaphragmatic defect. It is a rare malformation in adulthood because death commonly occurs within the first hours of life due to pulmonary hypoplasia and cardiorespiratory failure as the abdominal contents invade the chest, preventing the development of the fetal lung. The anomaly, originating in organogenesis, may result in diaphragm imperfection and can occur in various locations and sizes [
1].
Diagnosis of agenesis in asymptomatic adult patients with no history of trauma is quite complex. For such a diagnosis, clinical manifestations such as dullness to percussion and absence of vesicular murmur in a lung field must be taken into consideration [
2]. Failure of intercostal drainage on suspicion of pleural effusion or hemothorax should also be considered.
The greatest difficulty regarding the approach to large diaphragmatic defects centers around the issue of when, how, and whether to operate. Due to the danger of intestinal incarceration and strangulation, immediate repair is essential in cases of partial defects, including those in asymptomatic individuals. The requirement for surgical correction in cases of large diaphragmatic defects is discussed from another perspective, as the free space provides movement of the herniated viscera, offering a low risk of intestinal complications [
3].
Case Report
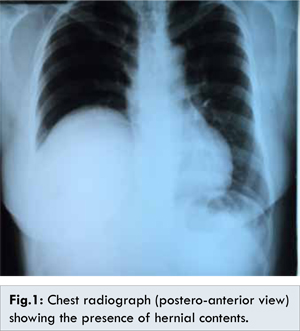
A 40-year-old female patient approached the outpatient service of the State Hospital of Porto Primavera, SP, Brazil, complaining of discomfort in the right hypochondrium and hemithorax radiating to the right scapular region. She was also intolerant to fatty foods. The patient reported no previous trauma or thoracic surgery, and her family history was normal. However, she reported having undergone three previous episodes of thoracentesis on diagnostic suspicion of right pleural effusion when she was treated for respiratory illnesses in an emergency situation. However, she did not produce any type of secretion in any puncture. A physical examination revealed a decreased right vesicular murmur, and the upper abdominal ultrasound report revealed cholelithiasis. Chest radiograph showed presence of hernia contents in thorax [Fig.1].
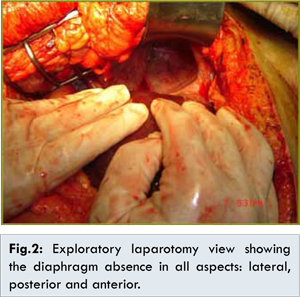
Surgical treatment consisting of a laparotomy with a Kocher incision was performed in a primary care hospital. During the inventory of the abdominal cavity, it was not possible to locate the gallbladder; therefore, the surgical procedure was terminated, and the patient was transferred to our hospital. The next day, the patient underwent an exploratory xiphopubic laparotomy. After releasing the hepatic ligaments, the intrathoracic liver was found to be elevated and rotated; when the organ was pulled into the abdominal cavity, it was possible to visualize the gallbladder and perform the cholecystectomy. The intraoperative findings included the absence of the right diaphragmatic dome with communication between the abdomen and right hemithorax [Fig.2].
At seven years of follow-up, the patient is asymptomatic with respect to the right diaphragmatic dome agenesis but presented a xiphopubic incisional hernia requiring surgical correction. On that occasion, with anesthesia control and tactical planning in mind, a thoracic tomography was performed which did not reveal any further findings regarding agenesis or any postoperative complications [Fig.3,4].
Discussion
In early pregnancy, the embryonic pleuroperitoneal membrane and transverse septum join to begin diaphragm formation. In the third week of gestation, the association of the transverse septum with the dorsal mesentery of the foregut gives rise to two openings in which the thoracic and abdominal contents meet. In the ninth week of pregnancy, these openings close [
4]. Thus, any process that prevents the closing of these channels can lead to defects in the diaphragm, including a congenital diaphragmatic hernia and diaphragmatic dome agenesis [
5].
Specifically, the pathogenesis of diaphragmatic dome agenesis is still not clear. Some evidence suggests that it occurs due to improper development of the multiple embryonic sources of the diaphragm (the transverse septum, peritoneal folds and the somites) [
6,
7].
In 1948, Bochdalek discovered the congenital diaphragmatic hernia that bears his name. The classic form of congenital diaphragmatic hernia is located on the left side in the posterolateral region of the diaphragm, and its occurrence on the right side is very rare and carries a worse prognosis. Reported cases of congenital diaphragmatic hernia on the right side include 8% to 15% of all cases [
8]. Several authors believe that congenital diaphragmatic dome agenesis is an extreme genre of congenital diaphragmatic Bochdalek hernia due to the similarities observed between the two. Congenital diaphragmatic dome agenesis is still the rarest form of congenital diaphragm malformation and is reported in 6% of all cases of congenital diaphragmatic hernia. Similar to a congenital diaphragmatic hernia, unilateral congenital diaphragmatic dome agenesis occurs more often on the left side than the right side, and the few reported cases of bilateral congenital diaphragmatic dome agenesis have exhibited extreme mortality [
8].
In neonates, the clinical course of diaphragmatic dome agenesis is well documented; however, there is little significant information regarding this condition in adulthood. Diaphragmatic dome agenesis is extraordinarily rare in adults because pulmonary hypoplasia leads to gradual respiratory failure and, consequently, to the death of the individual after birth. There are only three reported cases in the English literature [
9].
Chest X-ray or contrast upper gastrointestinal radiography (REED), computed tomography (CT), and magnetic resonance imaging (MRI) are the imaging modalities used to establish a diagnosis of diaphragmatic dome agenesis. In cases where patients have symptoms of obstruction due to an intrathoracic visceral hernia, chest X-rays are used to aid diagnosis. A CT scan of the chest and abdomen is necessary in cases of solid organ herniation or negative X-ray findings. CT and three-dimensional reconstruction are the most advanced resources currently available; however, even CT cannot be conclusive, and in some cases, it may be necessary to use sagittal or coronal MRI [
10].
Individuals suffering from congenital diaphragmatic dome agenesis can remain asymptomatic for decades. When symptomatic, early surgical intervention may prove beneficial for the patient. The issue of approach which should be adopted in adult patients with diaphragmatic agenesis is controversial. Often, those exhibiting right diaphragmatic dome agenesis do not require surgery because the liver prevents the occurrence of a visceral hernia. However, left diaphragmatic dome agenesis may more often require reconstruction. Patients presenting symptoms such as dyspnea, recurrent pleural effusion, or organ herniation require a surgical approach, regardless of the location of the defect. A thoracotomy in the fifth or sixth intercostal lateral space offers excellent access, although a transabdominal approach may be used if necessary. Reconstruction materials include free skin grafts, abdominal muscle grafts, and prosthetic material [
10].
In the case presented here, non-surgical correction of right diaphragmatic dome agenesis was selected because the patient was asymptomatic.
Conclusion
The gallbladder was successfully removed, and the patient has progressed favorably to date, with no medical problems related to the right diaphragmatic dome agenesis.
References
- Bhan V, Rajagopal P, Kumar K, Raghavendra KH. Agenesis of the hemidiaphragm: a rare presentation in an adult. Indian J Chest Dis Allied Sci. 2013;55:109-111.
- Wakai A, Winter DC, O’Sullivan GC. Unilateral diaphragmatic agenesis precluding laparoscopic cholecystectomy. J Soc Laparoendosc Surg. 2000;4:259-261.
- Fei L, Trapani V, Moccia F, Cimmino M. A rare case of left diaphragmatic agenesis in a elderly patient. Chir Ital. 2008;60:483-486.
- Karadeniz L, Guven S, Atay E, Ovali F, Celayir A. Bilateral diaphragmatic defect and associated multiple anomalies. J Chin Med Assoc. 2009;72:163-165.
- Ali SA, Haseen MA, Beg MH. Agenesis of right diaphragm in the adults: a diagnostic dilemma. Indian J Chest Dis Allied Sci. 2013;56:121-123.
- Jha A, Ahmad I, Naseem I. A rare case of partial diaphragmatic agenesis with thoracic liver herniation and anteriorly displaced intrathoracic kidney in an adult diagnosed by displaced diaphragmatic crus. Hernia. 2014;18:893-896.
- Merrell AJ, Kardon G. Development of the diaphragm - a skeletal muscle essential for mammalian respiration. FEBS J. 2013;280:4026-4035.
- Mirza B, Bashir Z, Sheikh A. Congenital right hemidiaphragmatic agenesis. Lung India. 2012;29:53-55.
- Medina CB, Pêgo-Fernandes PM, Jatene FB. Pneumotórax recidivante secundário à agenesia do diafragma. J Pneumol. 2002;28:48-50.
- Pousios D, Panagiotopoulos N, Argyriou P, Piyis A. Diagnosis and surgical management of diaphragmatic agenesis in an adult: report of a case. Surg Today. 2010;40:357-359.