Introduction
Cardiac perforation is a rare complication after pacemaker insertion (PMI) and the incidence is 0.1%-0.8% [
1]. The right atrium, being thinner than the right ventricle (RV), is prone to perforation by the pacemaker lead [
1]. Here we report a case of right ventricular perforation and pericardial tamponade after PMI, which required emergent pericardial window creation.
Case Report
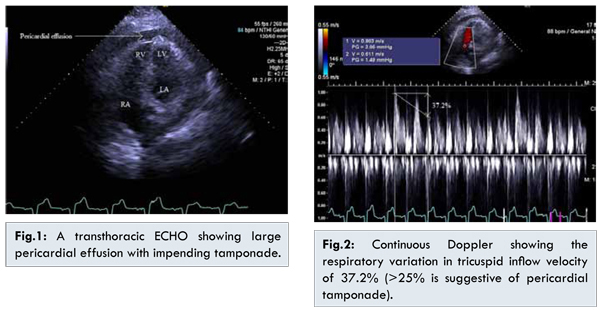
A 74-year-old, morbidly obese male (BMI 47.33 kg/m2) with hypertension, diabetes mellitus, heart failure with preserved ejection fraction (HFpEF), stage III chronic kidney disease (CKD), gastrointestinal (GI) bleed, atrial fibrillation (AF) and tachycardia-bradycardia syndrome presented with dyspnea, melena and dizziness. Prior hospitalizations include acute GI bleed due to nonsteroidal anti-inflammatory drugs (NSAIDs) induced gastric ulcerative lesions two months prior and permanent dual chamber PMI indicated for tachy-brady syndrome three weeks before current presentation. After the PMI, the patient was restarted on warfarin for AF, which was previously discontinued due to acute GI bleed. On admission, blood pressure (BP) was recorded at 61/26 mmHg, which minimally responded to intravenous (IV) fluid bolus. Systemic examination was unremarkable, except for the presence of distant heart sounds that were attributed to body habitus. Laboratory studies revealed an International Normalized Ratio (INR) of 2.2 and a hemoglobin (Hb) concentration of 8.17 gm/dL, which was a significant drop from baseline Hb of 12.1 gm/dL over three weeks. Stool fecal occult blood test (FOBT) was positive. Results of the other tests, including cardiac enzymes, electrocardiogram (ECG), and chest x-ray were unremarkable. Based on the presentation, treatment was directed towards the management of acute GI bleed. The patient was resuscitated with IV fluids, three units of packed red blood cells (PRBCs) and eight units of fresh frozen plasma (FFP). Esophagogastroduodenoscopy revealed duodenal erosions. Despite adequate resuscitation with IV fluids, PRBC transfusions, and FFP, hypotension persisted, which required administering vasopressors. Improvement in Hb was noted without improvement in patient’s condition and an echocardiogram (ECHO) was performed, which showed ejection fraction of 55% with large pericardial effusion and impending cardiac tamponade [Fig. 1,2]. The patient was transferred to a tertiary care facility, where repeat ECHO showed a large (>10 mm) circumferential pericardial effusion with evidence of cardiac tamponade, thrombus in the pericardial cavity overlying the RV, dilated inferior vena cava (3.1 cm) without respiratory variations, consistent with perforation of the RV at the site of PMI. The emergent pericardial window was created and 850 mL of blood and a large thrombus overlying the RV at the site of perforation were removed. Subsequent ECHO showed resolution of pericardial tamponade and patient was discharged in good health.
The widespread use of pacemaker implantation for the management of malignant arrhythmia is an evolution in cardiovascular medicine; however, complications arising from this life-saving procedure can be devastating. The incidence of cardiac perforation resulting from pacemaker insertion is 0.1%-0.8% [
2]; however, the consequences can be life-threatening, require a multidisciplinary approach, and high-risk cardiothoracic interventions. Cardiac perforation after pacemaker insertion can occur within twenty-four hours, within one month and after one month, which are termed as acute, subacute and chronic cardiac perforations, respectively [
1]. Compared to chronic cardiac perforation, acute cardiac perforation is more common [
3], carries worse prognosis and higher mortality [
2]. Risk factors for cardiac perforation and pericardial effusion include older age, female sex, low body mass index, corticosteroid use and the use of anticoagulants [
2,
4]. In addition to sensing failure, signs and symptoms of pacemaker lead perforation include chest pain, shortness of breath, syncopal episodes, muffled heart sounds, raised jugular venous pressure (JVP) and cardiogenic shock [
1]; however, approximately 15% of patients with pacemaker lead perforation remain asymptomatic and can only be detected by cardiac compound tomography (CT scan) [
2,
5]. A high index of suspicion is required for patients presenting with signs and symptoms of cardiac perforation after pacemaker insertion and initial diagnostic tests should include an EKG and a chest X-ray [
6], which could reveal low voltage tracing in addition to electrical alternans and pacemaker lead migration, respectively. The diagnosis of pacemaker lead perforation is confirmed by echocardiography with Doppler, which detects active lead screw or passive lead tip in the pericardial cavity [
4]. Cardiac CT scan remains the gold standard imaging modality of choice for detecting pacemaker lead migration even in asymptomatic patients [
5]. Management depends on the presence or absence of pericardial effusion and/or tamponade as the presence of pericardial effusion and/or tamponade requires emergent surgical intervention whereas perforation without tamponade or effusion requires simple fluoroscopic guided lead traction [
2].
The diagnosis of cardiac perforation induced by pacemaker insertion can sometimes be challenging, such as in our case, where hypotension and dyspnea were initially attributed to active GI bleed in consideration of recent hospitalization for duodenal ulcer, drop in hemoglobin and positive FOBT on admission. Risk factors for cardiac perforation, in our case, include older age and concurrent use of warfarin for the management of AF. Initial EKG and chest X-ray remained unremarkable; however, echocardiography with Doppler confirmed the presence of pericardial tamponade and a large thrombus overlying the RV in the pericardial cavity at the site of pacemaker lead perforation. The presence of pericardial tamponade required the life-saving emergent creation of a pericardial window.
Conclusion
Insertion of intracardiac devices is a life-saving procedure for the management of certain arrhythmias; however, the complication such as cardiac perforation can be life-threatening, even though it is infrequent. Clinical presentation can vary depending on the duration since pacemaker insertion and signs and symptoms include sensing failure, chest pain, shortness of breath, syncope, elevated JVP and cardiogenic shock. Echocardiography with Doppler remains the first-line diagnostic test of choice; however, cardiac CT scan is the gold standard method to detect pacemaker lead perforation even in asymptomatic patients. Management depends on presence or absence of pericardial effusion and/or tamponade. A high index of suspicion is required for patients presenting with dyspnea and hypotension after pacemaker insertion and the echocardiogram with Doppler should be obtained on presentation to recognize this life-threatening complication of pacemaker insertion.
References
- Banaszewski M, Stepinska J. Right heart perforation by pacemaker leads. Archives of Medical Science. 2012;8(1):11-13.
- Seil Oh. Cardiac Perforation Associated with a Pacemaker or ICD Lead. In: Das MK, editor. Modern Pacemakers - Present and Future. Available from: http://www.intechopen.com/books/modern-pacemakers-present-and-future/cardiac-perforation-associated-with-a-pacemaker-or-icd-lead. Accessed on November 6,2015.
- Cevik C, Wilborn T, Corona R, Schanzmeyer E, Nugent K. Post-cardiac injury syndrome following transvenous pacemaker insertion: A case report and review of the literature. Heart, Lung & Circulation. 2009;18(6):379-383.
- Ohlow MA, Lauer B, Brunelli M, Geller JC. Incidence and predictors of pericardial effusion after permanent heart rhythm device implantation: prospective evaluation of 968 consecutive patients. Circulation Journal. 2013;77(4):975-981.
- Mak GS, Truong QA. Cardiac CT: Imaging of and Through Cardiac Devices. Current Cardiovascular Imaging Reports. 2012;5(5):328-336.
- Santana-Cabrera L, Pérez-Acosta G, Manzanedo-Velasco R, Sánchez-Palacios M. Perforation of right ventricle with cardiac tamponade following pacemaker implantation. International Journal of Critical Illness & Injury Science. 2011;1(2):169-170.