Introduction
Post-traumatic arteriovenous fistulas account for 10% to 20% of all cases of traumatic vascular injury and result primarily from gunshot and stab wounds [
1-
3]. High-output heart failure due to post-traumatic aortocaval fistula is rare, unlike atherosclerotic abdominal aortic aneurysms [
4,
5]. In this paper, we represent a case of congestive heart failure that resulted from an ilio-caval fistula following a traumatic injury in a man with no prior cardiac disease.
Case Report
A 43 year old man sustained an isolated gunshot wound to his right lower quadrant where an urgent exploratory laparotomy was performed 23 years ago. Through and through injuries to the bowels were repaired primarily and no vascular trauma were recognized at that time. The patient presented after 23 years with symptoms of recurrent atrial fibrillation and congestive heart failure with intermittent claudication at the right lower extremity. On admission physical examination revealed a blood pressure of 130/80 mmHg, heart rate of 110 bpm, associated with irregular pulses and a loud abdominal bruit was detected in abdomen mainly at his right lower quadrant. EKG showed atrial fibrillation.
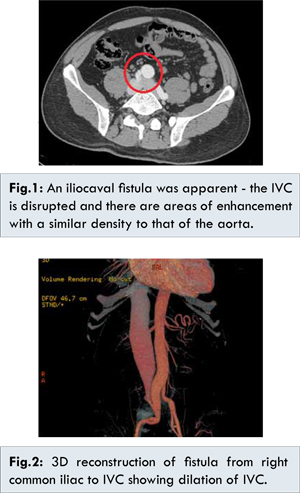
Conservative management was started waiting for further investigation. A transthoracic echocardiography was significant for low EF of 45% with global hypokinesia and no valvular diseases. Cardiac catheterization confirmed the high output failure, with high pulmonary pressure and a systemic pressure of 50 mm Hg. An abdominal Echo-Doppler showed a fistula at the right distal part of the common iliac artery communicating with the inferior venae cavae (IVC). A contrast enhanced CT scan confirmed these findings and showed a fistula of 8 mm diameter and 7.5 mm in length, a dilated IVC of 4.5 cm, a dilation of the right iliac artery pre-fistula of 2.4 cm and a diameter of 1.4 cm post fistula [Fig.1,2].
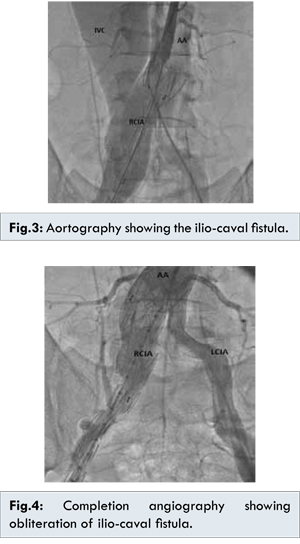
Taking into consideration the previous abdominal surgery and the chronicity of the arteriovenous fistula, an endovascular treatment was then discussed with the patient who agreed to proceed. A percutaneous approach was done through the left common femoral artery concomitant with a cut-down at the right inguinal area. A 5F pig tail graduated was percutaneously installed from the left CFA to opacify the aorto-iliac artery. Cut-down on the right side and a stent graft was deployed into the right common iliac artery. A post deployment angioplasty was done using a balloon with complete sealing of the fistula demonstrated by a completion angiography [Fig.3,4].
The patient had an uneventful postoperative course thereafter. Follow up CT scan showed obliteration of the fistula. At six month, the Doppler examination showed normal venous flow in the lower extremity, with no evidence of thrombus formation. The patient is currently 3 years post procedure without congestive heart failure symptoms or lower extremity pain, periodic duplex imaging has confirmed absence of flow in the fistula. Cardiac catheterization has not been repeated, but TTE has demonstrated normal cardiac function.
Discussion
Left unchecked, large-vessel arteriovenous fistulas can result in high-output congestive heart failure, and aneurysmal degeneration of the involved arterial and venous segments may also occur [
6,
7]. Cardiac decompensation occurs in about 75% of patients due to shunting of blood from a high-resistance arterial circuit to a low-resistance venous system. Elevated jugular venous pressure, tachycardia, and widened pulse pressure are common clinical signs. The increased cardiac preload, together with decreased afterload, leads to a compensatory increase in cardiac output and, possibly, heart failure [
7].
Until recently, open surgery was a traditional treatment, but mortality rate is high, ranging from 20%-50% according to previous reports [
8,
9]. In the present case, the arteriovenous fistula became symptomatic many years after the initial surgery, it manifested with signs of congestive heart failure and atrial fibrillation. It may be possible that the fistula developed secondarily, due to abrasion of the pulsating vessel walls. In contrast, it is also likely that a small arterial injury was missed at the time of initial injury and eventually decompressed into the inferior vena cava. Ultrasound revealed the vessel-wall defect rapidly. Endovascular placement of covered stents is the preferential treatment of arteriovenous fistula of the common iliac region at present.
Conclusion
Traumatic arteriovenous fistula is a rare entity and atrial fibrillation is a rarer manifestation of traumatic arteriovenous fistula. We have to always rule out any vascular lesions in patient with a history of trauma and abnormal abdominal heart sounds. Endovascular repair by stent-graft is one of the available options for the treatment of arteriovenous fistula combined with congestive heart failure and atrial fibrillation.
References
- Semiz E, Sancaktar O, Yalcinkaya S, Demircan A, Deger N, et al. Thoracic aortocaval fistula due to gunshotwound. Thorac Cardiovasc Surg. 1996;44:261-263.
- Duong C, Atkinson N. Review of aortoiliac aneurysms with spontaneous large vein fistula. Aust N Z J Surg. 2001;71:52-55.
- Lanne T, Bergquist D. Aortocaval fistula associated with ruptured abdominal aorticaneurysms. Eur J Surg. 1992;158:457-465.
- Burke AM, Jamieson GG. Aortocaval fistula associated with ruptured aortic aneurysm. Br J Surg. 1983;70:431-433.
- Reckless JPD, McColl I, Taylor GW. Aortocaval fistulae: an uncommon complication of abdominal aortic aneurysms. Br J Surg. 1972;59:461-465.
- Puppinck P, Chevalier J, Ducasse E, Smith M, Warembourg A, Coco B, et al. Connection between a long-standing traumatic arteriovenousfistula and development of aneurysmal disease. Ann Vasc Surg. 2004;18:604-607.
- Melliere D, Hassen-Khodja R, Cormier JM, Le Bas P, Mikati A, Ronsse H. Proximal arterial dilatation developing after surgical closure of long-standing posttraumatic arteriovenous fistula. Ann Vasc Surg. 1997;11:391-396.
- Brewster DC, Cambria RP, Moncure AC, Darling RC, LaMuraglia GM, Geller SC, Abbott WM. Aortocaval and iliac arteriovenous fistulas: recognition and treatment. J Vasc Surg. 1991;13:253-264.
- Woolley DS, Spence RK. Aortocaval fistula treated by aortic exclusion. J Vasc Surg. 1995;22:639-642.