Introduction
The term intestinal duplication cyst was used, for the first time by Fitz and its further classification was described by Gross in 1950. Enteric duplication cyst is a rare entity; it can appear in any part of alimentary tract from esophagus to rectum. Small bowel is the most common site of occurrence; however, colonic involvement is rare. Duplication cysts may remain asymptomatic or may present with abdominal pain, bleeding and obstruction [
1]. Resection of involved part of intestine is usually advised even in asymptomatic patients because of the high chance of perforation, obstruction, bleeding and rarely malignant degeneration.
Case Report
A 20 year girl presented with complaints of gradually increasing abdominal distension for 20 days, along with constipation, nausea and occasional bilious vomiting. She had past history of constipation, straining at defecation, sense of incomplete evacuation and abdominal fullness since the age of 3 years.
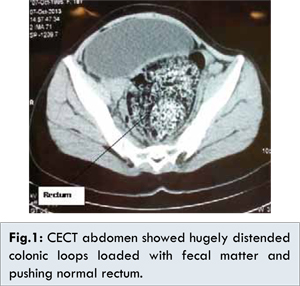
Abdominal examination revealed moderate abdominal distension, tenderness on deep palpation in the left iliac fossa and exaggerated bowel sounds. Hematological and biochemical investigations were unremarkable. Abdominal X-ray showed hugely distended sigmoid colon and other large bowel loops. Preoperative colonoscopy revealed a large globular, soft, cystic, sub-mucosal mass in rectum extending up to sigmoid colon about 15 cm along anterior wall of rectum which was almost completely obliterating the lumen. CECT abdomen showed hugely distended colonic loops loaded with fecal matter reaching up to levator ani level; rest of abdominal viscera were compressed and pushed to right side of abdomen [Fig.1]; right kidney was malrotated and enlarged, left kidney was not visualized. Uterus was bicornuate.
Initially a diagnosis of Hirschsprung’s disease was considered. She was adequately resuscitated and subjected to laparotomy, multiple colonic biopsies and appendectomy with loop ileostomy. Histopathology from multiple sites of large bowel and appendix showed adequate number of ganglion cells in between circular and transverse muscular layer thus ruling out presence of Hirschsprung’s disease; later on specimen biopsy also confirmed the findings of duplication in colon and adequate number of ganglion cells in distal sigmoid margin.
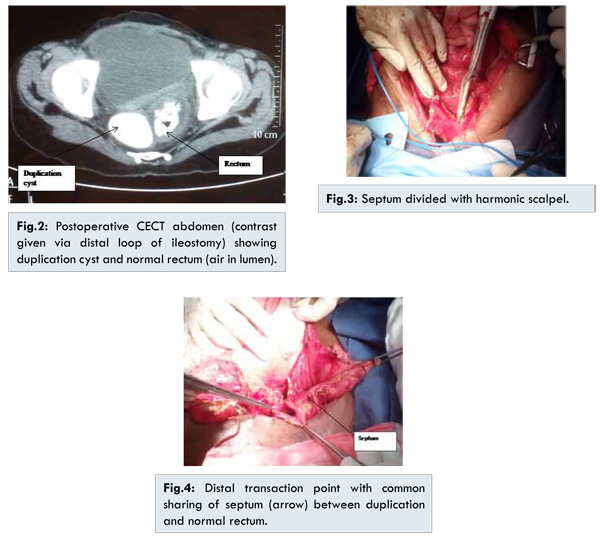
In postoperative follow up, she was reevaluated with CECT and contrast given via distal loop of ileostomy, revealed a normal caliber colon with an intervening septum (colonic duplication). The septum started in the ascending colon, was partial initially and then became complete and was extending along the entire length of colon, up to mid rectum (Levator ani level) where the duplication was terminating as a blind pouch and the normal lumen was opening into the anal canal [Fig.2]. At the second surgery done electively after 1 month of first surgery, it was found that the colon was hugely dilated and loaded with faecoliths from rectum to ascending colon. Colonic duplication was seen from the ascending colon to distal rectum. Subtotal colectomy, harmonic and stapler division of rectal septum of duplication cyst was done followed by an ascending colon and rectal anastomosis (side to end anastomosis with single layer interrupted 3-0 Vicryl) [Fig.3]. The proximal and distal transaction points were mid ascending colon and recto-sigmoid junction respectively, loop ileostomy was retained for diversion [Fig.4]. Stoma started functioning well from first postoperative day. Oral diet was well tolerated from second postoperative day. She was discharged on 12th postoperative day in satisfactory general condition. Stoma closure was done after 3 months and she was asymptomatic at follow up 6 month after surgery. She is on regular follow up.
Duplication of intestine is a rare entity. Ileum is the most common site of occurrence (60%) [
2]. Other organs like esophagus, duodenum, stomach and colon are involved in only 4%-18% of all cases [
1,
2]. Duplication cysts may be divided into foregut, small bowel and large bowel duplication cysts. Foregut duplication cysts may further consist of esophageal, bronchogenic and neurogenic cysts, depending on embryologic site of origin [
3]. 50%-70% foregut duplication cysts are enterogenous [
4] and only 7%-15% are bronchogenic [
5]. Bronchogenic cysts constitute 6%-15% of all primary mediastinal masses.
Grossly, duplication cysts may be cystic (86%) or tubular structures [
2]. Tubular type can be further distinguished into double barrel (80%) and Y-shaped (20%) duplication cysts, till now only 9 cases of Y-shaped duplication cyst of colon have been reported, about 50% of these cases were in teenagers. Usually spherical cysts are found to be closed and tubular cysts communicate with intestinal lumen in most of cases, where the cyst and intestinal lumen usually share a common wall; however, the communication between these two portions may or may not occur. Cyst wall is formed by one outer muscular layer and inner lining of gastric mucosa (50%) in most of cases; it may also be covered with mucosa of colon and rectum. These cysts are usually situated on the mesenteric aspect and share a common muscular wall and blood supply with the intestinal wall. Duplication cyst may also be associated with genitourinary, cardiovascular, vertebral and spinal anomalies [
15]; our case was also associated with right malrotated kidney and bicornuate uterus.
About 75% of intestinal duplication cyst present in the first two years of life and only 30% are diagnosed in newborn period. Till date only 100 cases of colonic duplication cyst have been reported [
6]. Complete colorectal duplication cyst is a very rare condition, only 3 cases have been reported [
7], this duplication cyst mainly occurs in younger and adult age group. Abdominal distension, pain, vomiting and abdominal mass are the most common presenting symptoms in infant and neonates, however, most of colonic duplication cyst remain asymptomatic and are not diagnosed until adulthood. Abdominal pain is the most common presentation [
8] followed by other clinical manifestations like obstruction, volvulus and lower GI bleeding [
6]. Cause of above symptoms may be compression of adjacent organs or direct effect of distension. Rarely abrupt hemorrhage may be the result of gastric mucosal ulceration, erosion of adjacent organs and vessels.
CECT is an initial and highly sensitive diagnostic modality, cysts appear as non-enhancing cystic masses, and addition of contrast enema can demonstrate colonic filling defect and luminal cyst communication with the large bowel. Colonoscopic findings of luminal communication with large bowel or extrinsic compression may raise a suspicion of colonic duplication cyst; however this fails to diagnose duplication cyst in a significant number of patients [
10]. EUS typically shows “Gut signature” which consist of multilayered wall, relatively hyperdense inner mucosa and outer hypoenhancing layer of smooth muscle, its lack of well-developed multilayer wall is due to degeneration and some degree of involution, however finding of double layered wall is seen only in 50% of patients. Peristalsis in cyst wall can also see be on EUS [
11]. There is no consensus regarding management; some authors suggest routine resection of colonic duplication cysts even in an asymptomatic patient, because of the risk of complications such as bleeding, perforation, obstruction and rarely, malignant degeneration [
1]. Laparoscopic resection of large bowel duplication cyst has been also been reported [
13]. Malignant transformation is very rare [
14]. Because of the common blood supply and the fact that the cyst wall is commonly fused along mesenteric border of bowel, it is usually difficult to resect duplication cysts in isolation without intestinal resection, however, resection of duplications alone has been reported [
12]. Our case was a double barrel tubular colonic duplication cyst with a very long septum extending from mid-ascending colon to distal rectum. Therefore, the intervening mucosal septum between the duplicated and non-duplicated colon was divided. A colo-rectal anastomosis between the ascending colon with the distal rectum was done.
Conclusion
Large bowel duplication intestinal cysts are uncommon anomalies, which mainly present in infancy and pediatric age group but may be seen in adults. Because of their rarity, a diagnosis of duplication cyst may not be initially considered when they present in adulthood in most situations patients are managed surgically due to potential risk of perforation bleeding, obstruction and malignant degeneration.
References
- Holcomb GW, Gheissari A, O’Neill JA, Shorter NA, Bishop HC. Surgical management of alimentary tract duplications. Ann Surg. 1989;209:167-174.
- Puligandla PS, Nguyen LT, St-VilD, Flageole H, Bensoussan AL, Nguyen VH. Gastrointestinal duplications. Journal of Pediatr Surgery. 2003;38:740-744.
- Diehl DL, Cheruvattath R, Facktor MA, Go BD. Infection after endoscopic ultrasound-guided aspiration of mediastinal cysts. Interact Cardiovasc Thorac Surg. 2010;10:338-340.
- Whitaker JA, Deffenbaugh LD, Cooke AR. Esophageal duplication cyst. Case report. Am J Gastroenterol. 1980;73:329-332.
- Snyder ME, Luck SR, Hernandez R, Sherman JO, Raffensperger JG. Diagnostic dilemmas of mediastinal cysts. J Pediatr Surg. 1985;20:810-815.
- Fotiadis C, Genetzakis M, Papandreou I, Misiakos EP, Agapitos E, Zografos GC. Colonic duplication in adults: report of two cases presenting with rectal bleeding. World J Gastroenterology. 2005;11:5072-5074.
- Sarpel U, Le MN, Morotti RA, Dolgin SE. Complete colorectal duplication. Journal of the American College of Surgeons. 2005;200:304-305.
- Choong CK, Frizelle FA. Giant colonic diverticulum: report of four cases and review of the literature. Dis Colon Rectum. 1998;41:1178-1185.
- Reiser-Erkan C, Erkan M, Ulbrich E, JorgNahrig, JorgKleeff. Cystic colon duplication causing intussusception in a 25-year old man: Report of a case and review of the literature. BMC Surg. 2010;23:19.
- Domajnko B, Salloum RM. Duplication cyst of the sigmoid colon. Gastroenterol Res Pract. 2009.2009:918401.
- Spottswood SE. Peristalsis in duplication cyst: A new diagnostic sonographic finding. Pediatr Radiol. 1994;24:344-345.
- Pinto VC, Moraes RV, Cardim WH. Duplication of the alimentary tract; report of a case. J Int Coll Surg. 1956:403-408.
- Park YA, Jung EJ, Han SJ. Laparoscopic resection of duplicated sigmoid colon under the guidance of intraoperative colonoscopy. Surgical Laparoscopy, Endoscopy and Percutaneous Techniques. 2005;15:299-301.
- Horie H, Iwasaki I, Takahashi H. Carcinoid in a gastrointestinal duplication. J Pediatr Surg. 1986;21:902-904.
- Karkera PJ, Bendre P, D’souza F, Ramchandra M, Nage A, Palse N. Tubular Colonic Duplication Presenting as Rectovestibular Fistula. Pediatric Gastroenterology, Hepatology & Nutrition. 2015;18:197-201.