|
|
|
|
|
High Dosage Insulin Therapy in Calcium Channel Blocker and Beta Blocker Overdosage
|
|
|
viagra cena lekaren viagra cena apoteka
Department of Intensive Care Medicine, Rashid Hospital, Dubai Health Authority, Dubai, United Arab Emirates. |
|
|
|
|
|
Corresponding Author:
|
Dr. Mohamed Shoaib
Email: shoaibmima@gmail.com
|
|
|
|
|
|
|
|
|
Received:
17-DEC-2015 |
Accepted:
08-MAR-2016 |
Published Online:
30-MAR-2016 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Beta-blockers and calcium channel blockers over-dosage have similar presentation with hypotension and bradycardia, with considerable overlap in treatment and are often refractory to resuscitation measures. A 15 years old female, previously healthy, presented to hospital 3 hours after ingestion of calcium channel blocker, ß-blocker and acetaminophen. The patient presented with abdominal pain, hypotension and sinus bradycardia after ingestion of 100 mg of amlodipine and 100 mg of nebivolol and 15 gm acetaminophen. Gastric lavage with activated charcoal was done in private hospital, but because of her hemodynamic instability she was transferred to our hospital. Fluid resuscitation failure and increasing requirement of vasopressors (nor-adrenaline) required her admission to intensive care unit. She was treated with N-acetyl cysteine in view of raised acetaminophen level, insulin infusion, glucose supplementation with continuous monitoring of potassium and blood glucose. After 48 hours patient was hemodynamic stable without vasopressor support and discharged. |
|
|
|
|
|
Keywords :
|
Abdominal Pain, Calcium Channel Blockers, Drug Overdose, Gastric Lavage, Hypotension, Insulin.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffa4120c0000008a04000001000500 6go6ckt5b5idvals|589 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Overdoses with cardiovascular drugs are associated with significant morbidity and mortality [1,2]. Beta blockers and calcium channel blockers have similar presentation with overlapping treatment and are often refractory to standard resuscitation measures [1]. They often have a similar presentation with bradycardia and hypotension [1,2].
Case Report
A 15 years old female, previously healthy, presented to Accident and Emergency after ingestion of mixed overdose of calcium channel blocker, ß-blocker and acetaminophen due to exam stress. The patient presented after three hours of ingestion of 100 mg of amlodipine and 100 mg of nebivolol and 15 gm acetaminophen with presenting symptoms of abdominal pain, hypotension and sinus bradycardia. The patient had gastric lavage with activated charcoal in private hospital but because of her hemodynamic instability was transferred to our hospital.
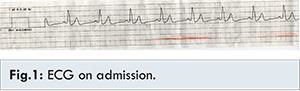
Patient was fully conscious, GCS 15/15, normothermic with systolic blood pressure of 68 mm Hg and mean pressure 43 mmHg, heart rate 42/min, respiratory rate 26/min, oxygen saturation 97% on nasal cannula. Electrocardiogram showed sinus bradycardia with wide QRS [Fig.1]. Fluid resuscitation failure and the need for increasing dosage of vasopressors required her admission to our intensive care unit (ICU). Hemodynamic monitoring through central venous pressure and invasive arterial blood pressure catheters was ongoing, and her baseline investigations were showing WBC count 19.10x103/µL (3.6-11.0) with neutrophilia 81% (55%-62%), hemoglobin of 12.7 gm/dL (11-15) and platelets count 29x103/µL (150-400).
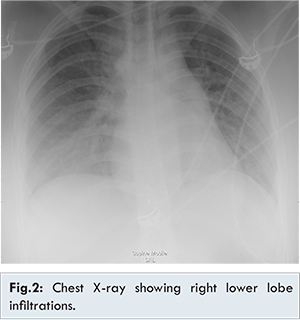
Cardiac BNP was 894 pg/mL (< 125), amylase 46 U/L (28-100 U/L), total bilirubin 1.5 mg/dL (0-1.0 mg/dL), troponin was negative and other liver and renal functions were normal. Her coagulation profile, urea and electrolytes, magnesium and phosphate were within normal range. Procalcitonin 0.72 ng/mL (less than 0.4) and lactic acid 3.5 mmol/L (0.5-2.2 mmol/L) were elevated. Chest X-ray show right lower lobe infiltrate mostly due to aspiration [Fig.2].
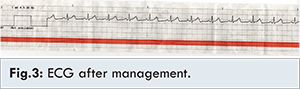
Acetaminophen level was elevated 73.40 µg/mL [10-30 µg/mL] with normal salicylate level. The patient was started on N-acetyl cysteine, blood gases showed metabolic acidosis mainly lactic acidosis inspite of high dosage of vasopressors, norepinephrine of 2 µg/kg/min and dopamine of 20 µg/min. Insulin infusion started with dose of 2 µg/kg/hr along with glucose supplementation aiming hyperinsulinemia-euglycemia with continuous monitoring of potassium and blood glucose to avoid the adverse effect of hypokalemia or hypoglycemia. Potassium replacement was needed and patient required a total of 200 mEq potassium over 48 hours. Restoration of the normal heart rate even before increase of the blood pressure was first sign of improvement, N-acetyl cysteine was discontinued when acetaminophen level become normalized <1.2 µg/mL. After 48 hours from insulin therapy initiation, the patient was hemodynamic stable, QRS normalized [Fig.3] after tapering of the vasopressors and so the insulin infusion was discontinued but with continuous monitoring of the glucose and potassium levels for 24 hours after insulin discontinuation.
Overdoses with cardiovascular drugs are associated with significant morbidity and mortality. Beta-blockers and CCBs represent the most important classes of cardiovascular drugs [1]. Beta-blockers and CCBs over dosage have similar presentation and treatment overlaps and are often refractory to standard resuscitation measures [1,2]. The common feature of beta-blocker toxicity is excessive blockade of the beta-receptors resulting in bradycardia and hypotension. Poisoning by CCBs is characterized by cardiovascular toxicity with hypotension and conduction disturbances, including sinus bradycardia and varying degrees of atrio-ventricular block [2,3]. Initial treatment is primarily supportive and includes saline fluid resuscitation which is essential to correct vasodilatation and low` cardiac filling pressures [4]. We illustrated in our case report that high dose insulin therapy along with glucose supplementation has emerged as an effective treatment for ß-blocker and calcium channel blocker poisoning. Our findings were in favor of Engebretsen KM, et al. article which stated the effectiveness of that treatment [4].
Shepherd G, et al. had showed that in recent review of 13 human cases of CCB poisoning, high dose insulin therapy appeared safe and provided clinical benefit in the 13 cases [5]. Megarbane B et al. illustrated in their work that the administration of high dose insulin produced cardiovascular stabilization, decreased the catecholamine vasopressor infusion rate and improved the survival rate in acute calcium channel antagonist and beta-blocker poisoning [6]. Stellpflug SJ, et al. reported a case of polydrug overdose involving nebivolol resulting in cardiac arrest successfully treated with high dose insulin infusion [7]. Nickson CP, recommended the use of high dose insulin euglycemia in CCB poisoning as initial therapy rather than as a last resort as an effective therapy for impaired cardiac contractility [8,9,10]. Boyer and Shannon reported 2 cases of CCB overdose were treated with insulin at 0.5 U/kg/hr
which rapidly reversed the cardiovascular collapse [11].
The major anticipated adverse events associated with high dose insulin are hypoglycemia and hypokalemia so both must be corrected prior to initiating the therapy and regularly monitored every 30 minutes and for up to 24 hours after discontinuation of high dose insulin [4,12]. The change in serum potassium concentrations reflects shifting of potassium from the extracellular to intracellular space rather than a decrease in total body stores [4,11,13].
Conclusion
This case illustrated that high dosage insulin therapy along with glucose supplementation has emerged as an effective treatment for ß-blocker and calcium channel blocker poisoning, and improved the survival rate. Hypoglycemia and hypokalemia are the major side effects so must be corrected prior to initiating the therapy and regularly monitored every 30 minutes and for upto 24 hours after discontinuation of high dose insulin.
References
- Shepherd G. Treatment of poisoning caused by beta-adrenergic and calcium-channel blockers. Am J Health Syst Pharm. 2006;63:1828-1835.
- Reith DM, Dawson AH, Epid D. Relative toxicity of beta-blockers in overdose. J Toxicol Clin Toxicol. 1996;34:273-278.
- Thakrar R, Shulman R, Bellingan G, Singer M. Management of a mixed overdose of calcium channel blockers, ß-blockers and statins. BMJ Case Rep. 2014 doi:10.1136/bcr-2014-204732.
- Engerbresten KM, Kaczmarek KM, Morgan J. High-dose insulin therapy in beta-blocker and calcium channel blocker poisoning. Clin Toxicol. 2011;49:277-283.
- Shepard G, Klein-Schwartz W. High dose insulin therapy for calcium channel blocker overdose. Ann Pharmacother. 2005;39:923-930.
- Megarbane B, Karyo S, Baud FJ. The role of insulin and glucose (hyperinsulinaemia/euglycaemia) therapy in acute calcium channel antagonist and beta-blocker poisoning. Toxicol Rev. 2004;23:215-222.
- Stellpflug SJ1, Harris CR, Engebretsen KM, Cole JB, Holger JS. Intentional overdose with cardiac arrest treated with intravenous fat emulsion and high-dose insulin. Clin Toxicol (Phila). 2010;48(3):227-229.
- Nickson CP, & Little M. Early use of high-dose insulin euglycaemic therapy for verapamil toxicity. Med J Aust. 2009;191(6):350-352.
- Greene SL, Gawarammana I, Wood DM, Jones AL, Dargan PI. Relative safety of hyperinsulinaemia/euglycaemia therapy in the management of calcium channel blocker overdose: a prospective observational study. Intensive Care Med. 2007;33(11):2019-2024.
- Kerns W 2nd. Management of beta-adrenergic blocker and calcium channel antagonist toxicity. Emerg Med clin North Am. 2007;25(2):309-331.
- Boyer EW, Shannon M. Treatment of calcium-channel-blocker intoxication with insulin infusion. N Engl J Med. 2001;344:1721-1722.
- Salhanick SD, Shannon MW. Management of calcium channel antagonist overdose. Drug Saf. 2003;26:65-79.
- Kambali S, Alalawi R, Nugent K. Prolonged refractory hypotension secondary to amlodipine overdose: a therapeutic challenge. ICU Director. 2013;4:136-142.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Ibrahim Shoaib M, Faoor Alrais Z, Elkhouly AHigh Dosage Insulin Therapy in Calcium Channel Blocker and Beta Blocker Overdosage.JCR 2016;6:135-138 |
|
Ibrahim Shoaib M, Faoor Alrais Z, Elkhouly AHigh Dosage Insulin Therapy in Calcium Channel Blocker and Beta Blocker Overdosage.JCR [serial online] 2016[cited 2026 Apr 7];6:135-138. Available from: http://www.casereports.in/articles/6/1/High-Dosage-Insulin-Therapy-in-Calcium-Channel-Blocker-and-Beta-Blocker-Overdosage.html |

|
|
|
|
|