Introduction
Fibroma or fibrothecoma (F/FT) represents most common benign sex-cord stromal tumors and accounts for 4% of all ovarian neoplasms [
1]. F/FTs are occasionally referred to by the common term “fibrothecomas” because of their histologic overlap [
2]. Their imaging features on CT and MRI have been evaluated in a lot of studies. Even now, however, radiologists often find it difficult to accurately diagnose these tumors [
3]; for example, differentiating them from uterine leiomyomas and Krukenberg tumors can be problematic.
Grossly, ovarian F/FTs represent unilateral tumors in about 90% of cases [
4]. Bilateral, multiple F/FTs are not common, and without recognition of their occurrence, a preoperative diagnosis could be more difficult. Besides, a secondary ovarian malignancy is typically bilateral rather than unilateral [
5], so bilateral ovarian F/FTs can be misdiagnosed as ovarian malignancies. Actually, to best of our knowledge, few case reports have presented imaging findings of bilateral and multiple ovarian F/FTs. Herein we describe a case of bilateral and multiple ovarian FTs.
Case Report
An 80-year-old woman with abdominal distention was admitted to our hospital for a workup for her abdominal masses, which had been detected on MRI. She had no history of malignancy. Laboratory tests showed CA 125 slightly elevated at 219.9 U/mL, while other tumor markers, CEA and CA 19-9, were within normal limits.
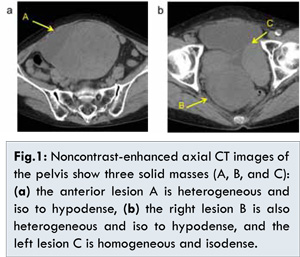
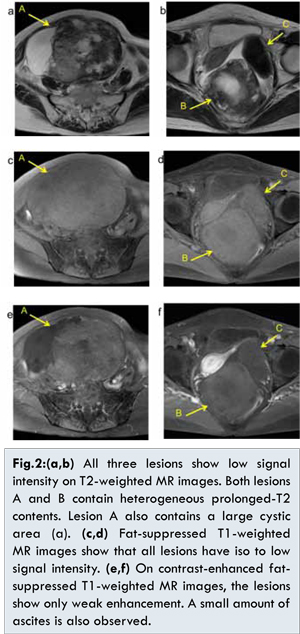
Noncontrast-enhanced CT revealed three well-demarcated solid masses in the pelvis. Both the anterior lesion of 20 cm diameter (lesion A) [Fig.1a] and the right lesion of 9 cm diameter (lesion B) [Fig.1b] showed heterogeneous and iso to hypo attenuation, whereas the left lesion of 7 cm diameter (lesion C) [Fig.1b] showed homogenous and iso attenuation. None of the lesions contained definite calcifications. In addition, small amounts of pleural effusion and ascites were detected. On T2-weighted MRI, all the lesions showed low signal intensity [Fig.2a and 2b]. Both lesions A and B also included heterogeneous portions showing high signal intensity, which might represent edematous or degenerative change. Lesion A also had cystic components on the periphery of the tumor. All masses showed iso to low signal intensity on fat-suppressed T1-weighted images [Figs. 2c and 2d]. Furthermore, they showed only weak enhancement on the contrast-enhanced images [Figs.2e and 2f]. No areas showing high signal intensity were detected on diffusion-weighted images (DWI). Considering that the right and left ovarian veins lead to lesion A and C, respectively, lesions A and C proved to originate from the right and left ovaries, respectively. Lesion B had continuity with broad ligament. Moreover, a cordlike structure was observed between lesions B and A, so these tumors were considered to originate in the right ovary, and both lesions were suspected of being twisted together. In addition, the uterine endometrium showed slight thickening for the patient’s age. On FDG-PET/CT, the lesions appeared to show no significant abnormal uptake of FDG. In this case, MR imaging suggested that all the lesions were F/FTs of ovarian origin. Therefore, bilateral salpingo-oophorectomy with total hysterectomy was performed.
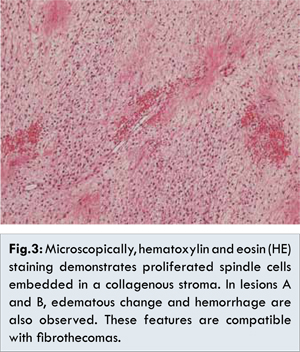
Intraoperative findings demonstrated that lesions A and B were indeed twisted together, with 540 and 360 degree rotations, respectively. However, the torsion demonstrated in both lesions was relatively loose and was easily released without discoloration of the fallopian tube. Macroscopically, the resected specimens of lesions A and B showed whitish elastic hard masses, indicating the tumor degeneration and hemorrhage. On the other hand, the specimen of lesion C showed a uniform and whitish elastic hard mass. The uterus was atrophic but did not contain any tumor. Microscopically, bilateral ovarian tumors were composed of proliferated spindle cells embedded in a collagenous stroma. In lesions A and B, edematous degeneration and intratumoral hemorrhaging were also observed. These pathological features were compatible with FTs [Fig.3].
The patient’s postoperative course was uneventful and she was discharged. The pleural effusion and ascites spontaneously resolved after the tumors were resected; the clinical course may suggest that the tumors might be associated with Meigs’ syndrome.
Discussion
Ovarian F/FT, the most common form of benign solid ovarian tumor, is characterized by spindle-shaped cells that resemble collagen-producing fibroblasts. The term “FT” is used when it is impossible to make a precise pathological distinction between the two pathological forms of fibroma and thecoma. The incidence of F/FT is 1 to 4% [
1,
5]. The median age is 45 (26-69) years, and 47.8% of patients are postmenopausal [
5]. The main presenting symptoms are abdominal pain and abdominal distention [
5]. Ovarian F/FT can be associated with ascites and pleural effusion, known as Meigs’ syndrome. Surgery is the recommended treatment for ovarian F/FTs, and conservative management should be undertaken with caution.
An accurate preoperative diagnosis is often difficult because of F/FT’s uncommon occurrence and its solid nature, which can mimic uterine fibroid or other malignant solid ovarian tumors. Ultrasound features of F/FTs are usually nonspecific, and MRI is often used to further differentiate ovarian F/FTs from other solid ovarian masses. To formulate an appropriate treatment, it is necessary to differentiate this disease from other disease entities presenting similar imaging findings. Many imaging characteristics for F/FT have been reported thus far. Among them, herein we discuss the four representative imaging findings of T/FT: hypointensity on T2WI, contrast enhancement, torsion, and hormonal activity.
Generally, differential diagnoses of solid adnexal tumors that can show hypointensity on T2WI include Krukenberg tumors, Brenner tumors, uterine fibroids, broad ligament leiomyomas, and ovarian F/FTs [
6]. Bilateral and multiple T2-shortening adnexal masses can lead to a misdiagnosis of Krukenberg tumor because a secondary ovarian malignancy is typically bilateral instead of unilateral [
5]. Among T2-shortening adnexal masses, an F/FT is generally unilateral and the incidence of multiple F/FTs of bilateral ovarian origin, as in this case, is relatively low: the incidence of multiple and bilateral ovarian Fs is about 10% [
5]. In the present case, multiple and bilateral lesions made the diagnosis more complicated to make. Few cases have been reported that discussed the detailed imaging findings of multiple F/FTs of bilateral ovarian origin. Moreover, in this case, two of the three lesions of F/FTs showed torsion themselves or with each other. So the two lesions of the right ovary showed atypical imaging findings because of the torsion, and the lesion of the left ovary showed the typical imaging findings. It is important to consider the possibility of F/FTs when we interpret bilateral, multiple adnexal lesions presenting with hypointensity on T2-weighted images.
It is also important to identify the degree of enhancement in a lesion after intravenous injection of contrast medium, because intratumoral edema or myxoid degeneration can increase F/FT signal intensity on T2WI. In the same way, intratumoral degeneration/degenerative change in F/FTs may show significantly less enhancement than in uterine myometrium and fibroids [
3]. In this case, all the lesions demonstrated only weak contrast enhancement, which was compatible with F/FTs. The two lesions of the right ovary showed mutual twisting, but the contrast enhancement was preserved. The pathological examination revealed that the twisting was so incomplete that the arterial inflow was not occluded. Therefore, the twist had little influence on the degree of contrast enhancement. It is essential to consider the enhancement features in order to differentiate the T2-shortening adnexal lesions. In cases complicated by torsion, the degree of enhancement should be interpreted carefully. However, the contrast enhancement of the lesion varies because the extent of torsion varies.
Cystic degeneration and hemorrhaging are common in F/FTs [
6]. The most commonly observed degenerative change in MR is the arrangement of the subcapsular cystic areas on the periphery of the lesion; this occurs most commonly in large F/FTs, such as those in our case [
3]. Moreover, in some case reports F/FTs exhibit hormonal activity. Increased levels of estrogenic activity demonstrate characteristic symptoms, such as atypical genital bleeding and imaging findings of thickened endometrium; therefore, these features may also be useful for the differential diagnosis.
Conclusion
In conclusion, we described a case of multiple FTs of bilateral ovaries. Although most cases of F/FTs occur unilaterally, we should recognize the bilateral, multiple occurrence of this etiology. When we discuss cases of bilateral T2-shortening adnexal lesions, F/FT should be considered for differential diagnoses.
References
- Montoriol PF, Mons A, lnes DD, Bourdel N, Tixier L, Garcier JM. Fibrous tumours of the ovary: aetiologies and MRI features. Clin Radiol. 2013;68:1276-1283.
- Chung BM, Park SB, Lee JB, Park HJ, Kim YS, Oh YJ. Magnetic resonance imaging features of ovarian fibroma, fibrothecoma, and thecoma. Abdom Imaging. 2014;40:1263-1272.
- Shinagare AB, Meylaerts LJ, Laury AR, Mortele KJ. MRI features of ovarian fibroma and fibrothecoma with histopathologic correlation. Am J Roentgenol. 2012;198:W296-303.
- Chechia A, Attia L, Temime RB, Makhlouf T, Koubaa A. Incidence, clinical analysis, and management of ovarian fibromas and fibrothecomas. Am J Obstet Gynecol. 2008;199:473.e1-e4.
- Leung SW, Yuen PM. Ovarian Fibroma: a review on the clinical characteristics, diagnostic difficulties, and management options of 23 cases. Gynecol Obstet Invest. 2006;62:1-6.
- Khashper A, Addley HC, Abourokbah N, Nougaret S, Sala E, Reinhold C. T2-hypointense adnexal lesions: an imaging algorithm. Radiographics. 2012;32: 1047-1064.