Introduction
Pilomatrixoma, also known as pilomatricoma or calcifying epithelioma of Malherbe, is benign neoplasm that is derived from hair follicle matrix cells. These lesions are typically found in the head and neck region, but also occur in the upper extremities and are rarely reported at other sites [
1]. The largest case series in the literature includes 346 pilomatrixomas of which 15.3% were observed in the upper extremities [
2]. We present a case of pilomatrixoma as a rare differential diagnosis of parotid swelling.
Case Report
A 21 year old female presented with six month history of insidious onset of an isolated swelling in front of left ear. The swelling was painless and slowly enlarging. She denied any history of trauma, fever, weight loss, difficulty in swallowing and snoring.
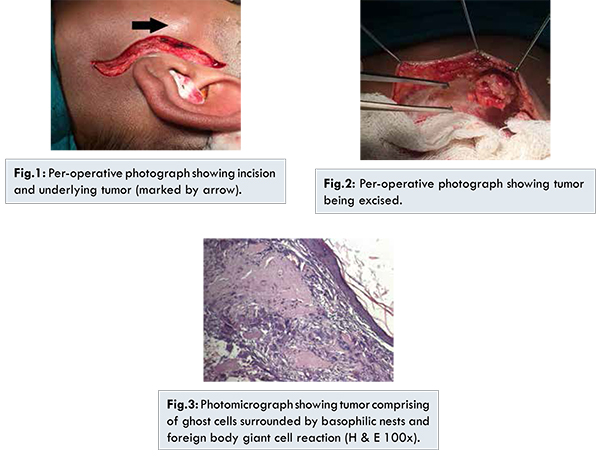
Physical examination revealed a 3x2 cm, non-tender hard mass fixed to the skin over the parotid region. It was superficial and non-mobile. There was no cervical lymphadenopathy. Oral examination was normal. Ultrasound demonstrated a well-defined echogenic mass with acoustic shadowing in the subcutaneous layer. Fine needle aspiration cytology was suggestive of mucoepidermoid carcinoma. Excision of tumor was planned. The mass was excised under general anesthesia via a lazy S incision, subplatysmal flaps were raised,mass of size 3.0 by 2.0 cm present over the superficial lobe of parotidwas dissected and excised completely. There was no involvement of parotid gland. On histopathology it was found to be a well demarcated tumor which was often surrounded by a connective tissue capsule, composed of islands of epithelial cells made of varying amounts of uniform basaloid material cells and showed cystic changes. These features were suggestive of benign tumor of epidermal appendages with differentiation towards hair follicle called as pilomatrixoma.
Pilomatrixoma, or calcifying epithelioma of Malherbe, is a benign skin neoplasm that arises from hair follicle matrix cells. In 1880, Malherbe and Chenantais first described this lesion referred to as the calcifying epithelioma, though it was thought to derive from sebaceous glands [
3]. The term pilomatrixoma was introduced in a publication by Forbis and Helwig in 1961 to better convey the histologic source [
4]. These lesions are typically found in the head and neck region, but have also been described in various upper extremity locations. These lesions present most commonly in children and young adults and they are noted more common in females.
A rare malignant counterpart, pilomatrix carcinoma, has been described, and approximately 90 cases have been reported in the literature. It is locally aggressive and can recur. In several cases, it has demonstrated metastases. Many key features are similar between these benign and malignant components; the primary differentiating characteristics include a high mitotic rate and atypical mitoses, central necrosis, infiltration of the skin and soft tissue, and invasion of blood and lymphatic vessels [
3,
5].
In this reported case, the definitive diagnosis was made after histologic examination following excision of the mass. Pilomatrixomas are often misdiagnosed on perioperative evaluation. In a series of 51 histologically proven pilomatrixomas, Wells et al. found that the referring diagnosis was incorrect in 94% of cases, and the perioperative diagnosis was incorrect in 57% [
6]. In a recent series of 346 pilomatrixomas, the preoperative diagnosis was accurate and consistent with the pathologic diagnosis of pilomatrixoma in 28.9% of cases [
2]. Incorrect preoperative diagnoses most commonly included unidentified masses, as well as epidermoid cysts, sebaceous cysts, dermoid cysts, non-specified cysts and foreign bodies.
Although pilomatrixomas are usually solitary, multiple lesions have been reported in association with genetic disorders, such as myotonic dystrophy, Gardner syndrome, xerodermapigmentosa and basal cell nevus syndrome. Diagnostic imaging is generally not obtained in the evaluation of patients with pilomatrixomas as they are usually small, superficial and well circumscribed. Plain radiographs in this case were unremarkable, but pilomatrixomas may demonstrate foci of calcification. Computed tomography demonstrates a sharply demarcated, subcutaneous lesion of soft tissue density, with or without calcification. MRI may reveal a rim enhancing lesion with small areas of signal dropout which may be consistent with calcifications. Ultrasound demonstrates a well-defined mass with inner echogenic foci and a peripheral hypoechoic rim or a completely echogenic mass with a strong posterior or acoustic shadow in the subcutaneous layer.
Conclusion
Pilomatrixoma can also be misdiagnosed as a mucoepidermoid carcinoma on aspiration cytology which is a rare finding in parotid region.
References
- Kumaran N, Azmy A, Carachi R, Raine PA, Macfarlane JH, Howatson AG. Pilomatrixoma - accuracy of clinical diagnosis. J Pediatr Surg. 2006;41:1755-1758.
- Pirouzmanesh A, Reinisch JF, Gonsalez- Gomez I, Smith EM, Meara JG. Pilomatrixoma: a review of 346 cases. Plast Resonstr Surg. 2003;112:1784-1789.
- Malherbe A, Chenantais J. Note sur1’ pithomecalcifi des glandes sabacees. Prog Med (Paris). 1880;8:826-828.
- Forbis R, Helwig EB. Pilomatrixoma. Arch Dermatol. 1961;83:606-618.
- Dutta R, Boadle R, Ng T. Pilomatrixoma carcinoma: case report and review of literature. Pathology 2001;33:248-251.
- Wells NJ, Blair GK, Magee JF, Whiteman DM. Pilomatrixoma: A common, benign childhood skin tumour. Can Surg. 1994;37:483-486.