Introduction
Primary endometrial squamous cell carcinoma is a rare entity. Usually squamous differentiation occurs in endometrioid type of carcinoma. Less than 100 cases of primary endometrial squamous cell carcinoma have been documented in literature. Frequency of squamous cell carcinoma is reported as 0.7% of endometrial carcinomas [
1].
Case Report
Fifty one year old post-menopausal lady presented with a history of discharge per vaginum for six months, for which no medical consultation was taken. The discharge was foul smelling, yellowish pus like material. Bleeding per vaginum which was irregular and scanty lasted for around one month. Initially she considered it as delayed periods as she attained menopause only recently (menopause less than one year). She consulted a gynecologist when she had a feeling of mass abdomen. She also had cough and dyspnea of recent onset at the time of admission. This was not associated with fever or expectoration. There was history of weight loss and loss of appetite. No history of hematuria, urinary retention, constipation, bowel disturbances, severe abdominal pain or vomiting was elicited.
General physical examination revealed pallor with normal vitals. Per abdomen a mass of fourteen week gravid uterus was palpable which was hard in consistency with smooth and regular borders and non-palpable lower bladder. Per vaginal examination revealed an ectocervix which was normal in appearance and consistency. A bimanual pelvic examination showed fourteen to sixteen week size gravid uterus. No adnexal mass, deposits in pouch of Douglas or palpable lymph nodes were noted. Chest examination showed bilateral coarse crepitations.
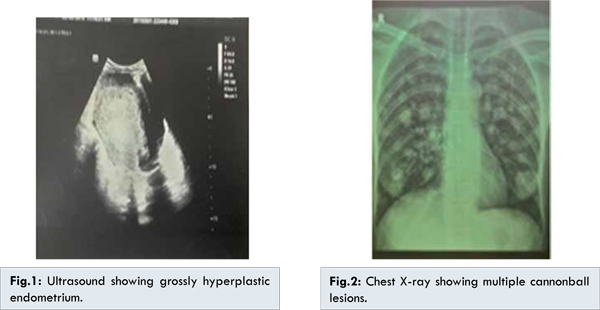
Ultrasonography of abdomen and pelvis showed an echogenic mass filling the uterus with minimal pyometra [Fig.1]. CT scan showed a uterine mass arising from uterine endometrium and multiple enlarged pelvic and para-aortic lymph nodes which had same echogenicity as the uterine lesion. Mantoux test was negative and ESR was normal. A pap smear was taken which was negative for intraepithelial malignancy. A differential diagnosis of uterine sarcoma or carcinoma endometrium was given. Her chest X-ray showed multiple cannon ball lesions bilaterally [Fig.2]. A fractional curettage of the endocervix and endometrium were done. The endocervical curetting’s were normal in histopathological examination. But histopathological examination of endometrial curettings revealed squamous cell carcinoma keratinising type endometrium. Primary surgery was not done in view of the extensive secondaries in the lung. After discussing with the radiotherapy department we planned for a palliative chemoradiation to alleviate her symptoms. Other supportive measures were also given. But patient died within three months of treatment due to respiratory insufficiency.
Diagnosis of primary squamous cell endometrial carcinoma requires exclusion of cervical squamous carcinoma extension and squamous cell differentiation of endometrioid type of carcinoma endometrium. In this case cervix was normal clinically with negative pap smear. Pathologist confirmed primary endometrial squamous cell carcinoma with no evidence of endometrioid adenocarcinoma in the specimen.
A differential diagnosis of tuberculosis was considered due to multiple cannon ball lesions in the lung and recent symptom of cough with dyspnoea. But Mantoux test was negative and ESR was normal. Other differential diagnosis which needed exclusion were uterine sarcoma and pulmonary leiomyomata secondary to benign metastasizing uterine leiomyomata. These were excluded after histopathological examination. Thus, diagnosis of primary endometrial squamous cell carcinoma was made.
The presence of squamous epithelium in the endometrium is variously termed as icthyosis uteri (condition in which endometrium is replaced by keratinised squamous epithelium) [
2]. Invasive squamous cell carcinoma endometrium is very rare and is thought to arise by one of the two mechanisms: upward spread of primary cervical lesion or transformation of reserve or stem cells positioned between glandular basement membrane and endometrial columnar epithelium. Invasive squamous cell carcinoma as a result of upward spread from cervix is unlikely here as cervix is normal. A final diagnosis of primary squamous cell carcinoma endometrium was made.
The immunohistochemical study of endometrium sample obtained from dilatation & curettage of uterus will be beneficial to the understanding of the clinicopathologic features of endometrial carcinoma before operation. According to Yao YY et al. and Alvarez T et al. the value of estimating the prognosis using the expressions of ER (oestrogen receptor), PTEN, P53 and Ki-67 was negative except for expressions of PR (progestin receptor) [
3]. Squamous cell carcinoma endometrium often show WT-1, cyclin D1 amplification, HER-2 over expression and/or amplification [
4]. Endometrial squamous cell carcinoma usually occurs in postmenopausal women. In contrast to type-1 endometrial adenocarcinoma, primary squamous cell carcinoma endometrium is not hormonally sensitive suggesting a unique pathogenesis [
5]. There is strong association with cervical stenosis, pyometra, chronic inflammation, nulliparity. Our case was 51 year old postmenopausal lady with history of one caesarian section and had minimal pyometra.
In endometrial carcinoma presence of a malignant squamous cell component worsens the prognosis. In endometrial squamous cell carcinoma, survival rate was 80% with stage 1, 20% with stage 3 and none with stage 4. No final treatment recommendation has been given so far. Therapy usually consist of hysterectomy plus adenexectomy and radiotherapy. In our case as there was extensive pelvic and paraaortic lymph node involvement, multiple cannon ball lesions in chest and treatment was decided as palliative radiation.
Conclusion
Endometrial squamous cell carcinoma is rare and aggressive malignancy seen in postmenopausal women. Mortality is often high due to delayed diagnosis.
References
- Terada T, Tateoka K. Primary pure squamous cell carcinoma: a case report. Int J Clin Exp Pathol. 2013;6(5):990-993.
- Bagga PK, Jaswal TS, Dutta U, Mahajan NC. Primary endometrial squamous cell carcinoma with extensive squamous metaplasia and dysplasia. Indian Journal of Pathology and Microbiology. 2008;51(2):267-268.
- Yao YY, Xu WZ, Wang Y, Shan DH, Wang TL, Wei LH. Relationship between the molecular biomarkers and clinicopathologic features and prognosis in endometrial carcinoma. Bejing Da Xue Xue Bao. 2011;43(5):743-748.
-
Alvarez T, M
iller E, Duska L, Oliva E. Molecular profile of grade 3 endometrial carcinoma - is it a type 1 or type 2 endometrial carcinoma? Am J Surg Pathol. 2012;36(5):753-761.
- Bures N, Nelson G, Duan Q, Maglicocco A, Demtrick D, Duggan MA. Primary squamous cell carcinoma endometrim: clinicopathologic and molecular characteristics Int J Gynecol Pathol. 2013:32(6):566-575.