|
|
|
|
|
Synovial Sarcoma of the Head and Neck: A Report of 2 Cases
|
|
|
benadryl pregnancy nausea benadryl and pregnancy ventolin over the counter nsw ventolin side effects
Department of Otolaryngology, Head and Neck; King George Medical College, Lucknow 226003, Uttar Pradesh, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Ritu Gupta
Email: ritugupta111@gmail.com
|
|
|
|
|
|
|
|
|
Received:
31-OCT-2015 |
Accepted:
04-MAR-2016 |
Published Online:
20-MAR-2016 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Synovial sarcoma is a rare malignant tumor which arises from a mesenchymal precursor stem cell that is unrelated to mature synovial tissue. Synovial sarcoma mostly affects extremities usually lower limbs between the ages of 15 and 40 years and the proportion of male-to-female patients is 3:2. It is very rare in the head and neck region especially in laryngopharynx. Till date, only six cases of synovial sarcoma involving laryngopharynx have been reported in the literature. Painless mass, hoarseness, upper respiratory distress, and dysphagia characterize the original complaints in laryngopharyngeal synovial sarcoma. Because head and neck synovial sarcoma in clinical practice is so uncommon, early diagnosis is difficult and the treatment protocol is unclear. The authors report two rare cases of synovial sarcoma of head and neck. First case was synovial sarcoma of larynx was treated by complete excision via the laryngofissure approach followed by radiotherapy. There has been no recurrence after 2 years of the complete excision and serial punch biopsies have come out to be negative. The second case is synovial sarcoma of the parotid treated by radiotherapy. |
|
|
|
|
|
Keywords :
|
Hoarseness, Larynx, Neck, Neoplasm Recurrence, Synovial Sarcoma.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffc8e30b0000007204000001000600 6go6ckt5b5idvals|586 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Synovial sarcoma is a mesenchymal malignancy of unknown histogenesis and occurs mostly in the extremities. Mainly young adults and adolescents are affected with a male female ratio of 3:2 [1]. The neoplasm often originates in proximity to the major joints, particularly the lower limbs, while other localizations, such as the retroperitoneum [2], pleura, lung [3,4], thorax and mediastinum [5] are unusual sites. Synovial sarcoma of head and neck are very rare and account for only 3% to 9% of all sarcomas [6,7]. The first case of synovial sarcoma of the neck was reported by Jernstrom in 1954 [8-10] since then only about 85 cases have been reported [6,8]. Two different histological types have been identified and are generally referred to as the classic biphasic type which is composed of epithelial cells and a spindle cell with a growth pattern which may be either glandular or solid, and a monophasic type in which a single cellular component is dominant; furthermore, other histological types of synovial sarcoma exist which are poorly differentiated and have a much lower incidence. The case is reported of a monophasic synovial sarcoma of the hypopharynx and the clinical and pathological features of this rare neoplasm are described stressing upon the management strategy of such cases.
Case Reports
Case 1
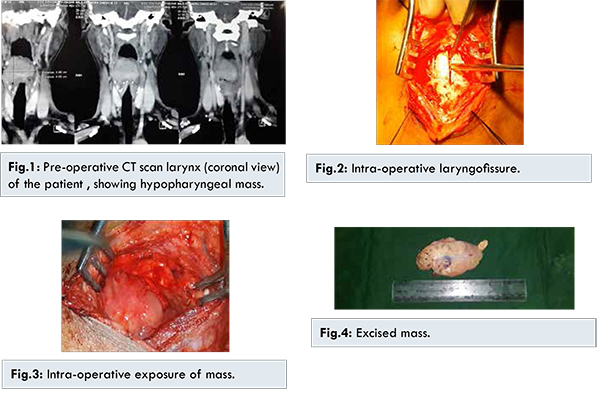
A 25 year old male presented with globus sensation in the throat with some swallowing difficulty since last 6 months. The patient also presented with a muffled voice of the same duration. There was no history of respiratory distress or any associated hemoptysis or hematemesis. On physical examination of the neck, no nodal hypertrophy or metastasis or neck mass was found. On indirect laryngoscopy a large space occupying mass in the supraglottis was seen which occluded any further view. Fibreoptic laryngoscopy revealed a huge pale mass with smooth surface. X-rays reveal no long bony metastasis. Punch biopsies returned negative results on prior two occasions. Chest X-rays were normal. CT scans show a hypo-pharyngeal neoplastic mass with preserved plane of cleavage with laryngeal walls, the size of the mass being 4.95x4.05 cm [Fig.1].
An elective tracheostomy was performed and general anaesthesia was administered through the tracheostomy. The anterior laryngofissure was performed for exploring the paraglottic region by raising the subplatysmal flaps with dissection through the strap musculature to expose the laryngeal framework and the proximal trachea. A laryngofissure was then made through the thyroid cartilage to the first tracheal ring and included the anterior commissure [Fig.2,3]. For optimal visualization of the larynx, a separate tracheotomy incision was created to place the endotracheal tube. The whole mass was excised leaving behind disease free margins. After complete excision, the mass was found to be 9x5 cm in dimension [Fig.4]. The base of the tumor was then chemically cauterized by silver nitrate. The wound was closed in layers and the specimen was sent for histopathological examination. Post-operative course was uneventful and the tracheostomy wound was closed on the tenth day. Biopsy report suggests, gross white polypoid mass having outer surface as glary and mucoid. Multiple sections from the growth show variegated appearance. Few areas show whitish nodular discoloration and calcification. In microscopic examination section shows monophasic synovial sarcoma. Post-operatively laryngoscopy was done which showed no residual disease. Punch biopsies were taken from the base area and the histopathological testing revealed no infiltration.
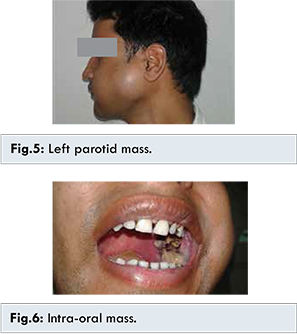
A 20-year-old male presented with two months history of a progressive swelling in the left parotid region. Patient gave history of intra-oral incision by some quack 1 month back which was followed by protusion and expansion of the mass intra-orally. Physical examination revealed a firm mass 7x6 cm, associated with local facial pain [Fig.5]. Intra-oral examination revealed ulcero-fungative growth coming out of the incision from the left buccal mucosa [Fig.6].
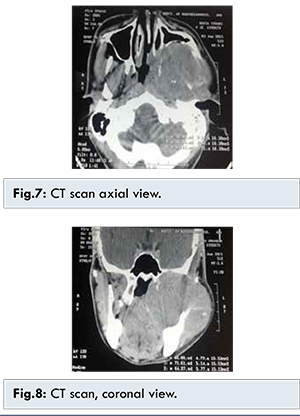
CT scan revealed ill-defined heterogeneously enhancing soft tissue attenuation lesion 7x6x5 cm in the left masticator space extending from the base of skull to the hyoid, medially from the nasopharynx to the infiltration of the left temporalis muscle laterally. The lesion was seen causing erosion of mandible, pterygoid plate, lateral wall of the maxillary sinus [Fig.7,8]. Fine needle aspiration cytology suggested malignant spindle cell neoplasm. Immunohistochemistry was positive for Vimentin and TLE-1, focally positive for EMA (epithelial membrane antigen) and negative for Pan-CK and p-63. Histology report said fragments of mucosal tissue lined by stratified squamous epithelium and sub-epithelial zone shows tumor disposed in sheets. The tumor is composed of spindle cells with pale cytoplasm and moderately pleomorphic elongated to ovoid nuclei with finely dispersed chromatin. Mitoses are frequent. Histomorphology and immunochemistry were consistent with synovial sarcoma. The patient was treated by radiotherapy (total dose 50 Gy).
Synovial sarcoma is a malignant soft-tissue neoplasm that arises from primitive pluripotential mesenchymal cells near to or remote from articular surfaces [1]. Although these tumors occur mostly in the extremities, they are also known to arise in the head and neck region [6,7,10]. The first description of a head and neck synovial sarcoma of hypopharynx was given by Jernstrom [9] in 1954. Synovial sarcoma have been described in hypopharynx, prevertebral and parapharyngeal areas, pharyngeal, laryngeal, nasopharynx, soft palate, tongue, maxillofacial region, mandible corner, sternoclavicular region, scapular region and the cervical oesophagus [11].
The most common parotid gland tumor is pleomorphic adenoma (60%) followed by Warthin adenoma (5-15%). In malignant neoplasms, the largest percentage is represented by mucoepidermoid carcinoma (8-15%) followed by adenoid cystic carcinoma (5%). Nonepithelial tumors like hemangioma are generally benign. However lymphoma, neuromas, neurofibromas, lipomas and sarcomas are also seen. Synovial sarcoma (SS) is the fourth most common variety of sarcoma after malignant fibrous histiocytoma, liposarcoma and rhabdomyosarcoma [12,13]. Synovial sarcoma classically affects patients between the ages of 15 and 40 years [14], and the proportion of male-to-female patients is 3:2 [15]. Histologically, synovial sarcomas are classified into monophasic epithelial, monophasic fibrous and biphasic and poorly differentiated variants. Monophasic type consists of single cellular type i.e., epithelioid or spindle cells both staining positive for cytokeratin and epithelial membrane antigen (EMA). The biphasic type has predominant spindle cells component with mast cells, mitosis, areas of calcification and scanty collagen. The epithelioid cells from pseudo-glandular cavities filled with mucin, which stain positive with Alcian blue, mucicarmine and periodic acid Schiff (PAS) stains. The difference between epithelioid and spindle cell component is done by Vimentin, a mesenchymal marker. Vimentin stains positive with spindle cells and negative with epithelioid type.
Poorly differentiated synovial sarcoma grows rapidly with infiltrative margins, showing haemorrhage and necrosis. It is considered as a form of progression, with a more aggressive behavior and a higher percentage of metastases [10]. Primary surgical excision is the mainstay of treatment. Postoperative radiation therapy is reserved for residual or recurrent disease [16]. Postoperative radiotherapy is supposed to decrease the probability of local recurrence. Chemotherapy is to reduce the number of remaining microscopic cells. The role of chemotherapy is controversial and debatable.
Conclusion
We present the above cases as synovial sarcoma in the head and neck. These are rare entities with synovial sarcoma of the pharynx being rarer, with less than ten cases reported in the literature.
References
- Perez CA. Unusual nonepithelial tumors of head and neck. Principles and practice of radiation Oncology. 1998;43:1125-1134.
- Shmookler BM. Retroperitoneal synovial sarcoma. A report of 4 cases. Am J Clin Pathol. 1982;77:686-691.
- Gaertner E, Zeren H, Fleming MV, Colby TB, Travis WD. Biphasic synovial sarcomas arising in the pleural cavity. A clinicopathologic study of five cases. Am J Surg Pathol. 1996;20:36-45.
- Zeren H, Moran CA, Suster S, Fishback NF, Koss MN. Primary pulmonary sarcomas with features of monophasic synovial sarcoma. A clinicopathological, immunohistochemical and ultrastructural study of 25 cases. Human Pathol. 1995;26:474-480.
- Witkin GB, Miettinen M, Rosai J. A biphasic tumor of the mediastinum with features of synovial sarcoma. Am J Surg Pathol. 1989;13:490-499.
- Bukachevsky RP, Pincus RL, Shechtman FG, Sarti E, Chodosh P. Synovial sarcoma of the head and neck. Head Neck. 1992;14:44-48.
- Pruszczynski M, Manni JJ, Smedts F. Endolaryngeal synovial sarcoma: case report with immunohistochemical studies. Head Neck. 1989;11:76-80.
- Dei Tos AP, Dal Cin P, Sciot R, Furlanetto A, Da Mosto MC, Giannini C, et al. Synovial sarcoma of the larynx and hypopharynx. Ann Otol Rhinol Laryngol. 1998;107:1080-1085.
- Jernstrom P. Synovial sarcoma of the pharynx: report of a case. Am J Clin Pathol. 1954;24:957-961.
- Weiss SW, Goldblum JR. Malignant soft tissue tumors of uncertain type. In: Enzinger and Weiss’s Soft Tissue Tumors, 5th ed. St. Louis, Mo: Mosby, 2008, pp 825-901.
- Doval DC, Kannan V, Mukherjee G, Shenoy AM, Shariff MH, Bapsy PP. Synovial sarcoma of the neck. Eur Arch Otorhinolaryngol. 1997;254:246-250.
- Seifert G, Sobin LH. Histological typing of salivary gland tumours. WHO, International Histological Classification of tumours. 2nd Edition Berlin: Springer-Verlag; Berlin.1991: pp.11-38.
- Sachse F, August C, Alberty J. Malignant fibrous histiocytoma in the parotid gland. Case series and literature review. HNO. 2006;54:116-120.
- Onerci M, Sarioglu T, Gedikoglu G, et al. Synovial sarcoma in the neck. Int J Paediatr Otorhinolaryngol. 1993;27:79-84.
- Gatti WM, Strom CG, Orfei E. Synovial sarcoma of the laryngopharynx. Arch Otolaryngol.1975;101:633-636.
- Amble FR, Olsen KD, Nascimento AG, Foote RL. Head and neck synovial cell sarcoma. Otolaryngol Head Neck Surg. 1992;107:631-637.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Nath K, Gupta R, Agarwal SP, Kumar SSynovial Sarcoma of the Head and Neck: A Report of 2 Cases.JCR 2016;6:124-128 |
|
Nath K, Gupta R, Agarwal SP, Kumar SSynovial Sarcoma of the Head and Neck: A Report of 2 Cases.JCR [serial online] 2016[cited 2026 May 17];6:124-128. Available from: http://www.casereports.in/articles/6/1/Synovial-Sarcoma-of-the-Head-and-Neck.html |

|
|
|
|
|