Introduction
Congenital epulis (CE), also known as congenital granular cell tumor (CGCT), is a rare benign tumor of newborns that was first described by Neumann et al. in 1871 [
1]. Epulis means swelling on the gingiva, and currently, the accepted terminology for epulis in the literature is a “congenital epulis of newborn”. A CGCT is mostly seen on the alveolar ridge of the maxilla or mandible, tongue, skin and soft tissue, and is generally a solid polypoid tumor [
2]. The incidence of CGCT is reported as six per million and is more common in female fetuses [
3]. CGCT is generally diagnosed during the third trimester of pregnancy as early as the 26th gestational week [
4]. These rare tumors may produce neonatal emergency situations such as airway obstructions or feeding problems [
5]. Surgical excision is the preferred treatment choice for a CGCT.
Although approximately 250 cases of CE have been reported, no cases have been reported from Turkey. Therefore, we would like to report a case of a CE diagnosed during the prenatal period from a reference hospital in Turkey.
Case Report
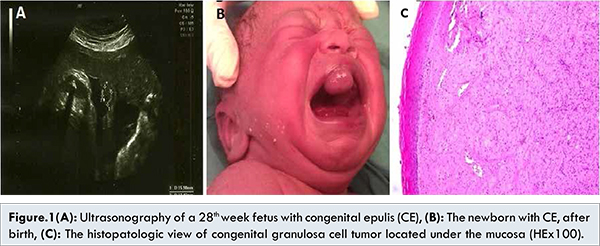
A 36-year-old woman at the 36th week of pregnancy was admitted to the outpatient antenatal care unit of Akdeniz University Hospital. Her obstetrical history revealed single living child delivered by Cesarean section. She had no history of systemic diseases or obstetric problems during her routine antenatal follow-up examinations. However, an antenatal ultrasonography at the 28th week of pregnancy revealed a congenital solid mass that was 16x11x12 mm in diameter on the anterior oral cavity of the fetus. On admission, ultrasonography revealed a hyperechoic solid mass of the same diameter in the oral cavity [Fig.1A]. The amniotic fluid was within normal ranges. A 3,480 gram female infant was born with Cesarean section with Apgar scores of 9/10 at 1/5 minutes, respectively. She had no signs of respiratory distress or airway obstruction. However, she had an oral mass that was 15x10x12 mm in size originating from the gingival region of the anterior maxillary alveolar ridge in the midline of the oral cavity [Fig.1B]. During the physical examination no other abnormalities were detected and she was referred to the Neonatal Care Unit. After receiving written informed consent from the parents, the solid mass in the oral cavity was removed by pediatric surgeons. The newborn tolerated the surgery well and on the third day she began breastfeeding. The pathologic examination of the tissue revealed homogenous solid sheets of large cells with eosinophilic granular cytoplasm and small round nuclei [Fig.1C]. The baby was discharged on the fifth day and regular check-ups revealed no evidence of recurrence.
This article described a CE case in a fetus diagnosed perinatally. CE, rare tumor in the oral cavity, is generally single tumor, although multiple lesions associated with nasal septum abnormalities have also been reported. The size of the tumor can vary from several millimeters to several centimeters [
6]. The female preponderance of 8:1 has been reported and the diagnosis is generally made by characteristic clinical findings after birth. There are conflicts in the pathogenesis of CE including endogenous hormones, trauma, and local metabolic or reactive changes [
7]. However, the exact pathogenesis cannot be reported yet. Prenatal diagnosis is also possible in the third trimester of the pregnancy with the help of ultrasonography or magnetic resonance imaging (MRI). A differential diagnosis should be made from other oropharyngeal masses such as teratoma, hemangioma, lymphangioma, and neurofibroma [
8]. The tumor location, sonographic appearance, presence at birth, and no malignant transformation aid in the differential diagnosis. Furthermore, teratomas usually contain calcifications and hemangiomas arise externally from subcutaneous tissues. The differential diagnosis from the adult type of granular cell tumor may be difficult. CGCTs can easily be differentiated from adult type GCTs by location, patient’s age, solid growth pattern, attenuated overlying epithelium, pericystic proliferation, and negativity of the lesion to S-100 immunohistochemical staining. With prenatal ultrasonography, polyhydramnios can be seen due to fetal swallowing defects. Although the spontaneous resolution of the tumor has been reported [
9], surgical resection is the preferred treatment choice. After surgical removal, no recurrence or malignant transformation has been reported, even in cases of incomplete excision [
7].
In our case, the fetus was a female with a single oral mass which was prenatally diagnosed with ultrasonography in the third trimester. The mass size did not grow and was easily removed after birth without any complications. Although the clinical characteristics were helpful for differential diagnosis in our case, the histopathological and immunohistochemical examinations confirmed our diagnosis. The prognosis of our case was good during the follow-up period, similar to the results in the literature.
In conclusion, further research should be performed to explain the exact etiology and growth of these lesions to avoid neonatal emergency situations. Physicians should pay special attention to the third trimester ultrasonography and examination of the face and oral cavity. In case of a suspicion of a lesion similar to CE, pregnant females should be referred to a multidisciplinary center for the delivery and management after delivery.
Acknowledgement
English of the manuscript was edited by American Manuscript Editing Service,
www.americanmanuscripteditors.com.
References
- Neumann E. Ein fall von kongenitaler epulis. Arch Heilkd. 1871;12:189-190.
- Conrad R, Perez MCN. Congenital Granular Cell Epulis. Arch Pathol Lab Med. 2014;138:128-131.
- Bosanquet D, Roblin G. Congenital epulis: a case report and estimation of incidence. Int J Otolaryngol. 2009;2009:508780.
- Nakata M, Anno K, Matsumori LT, Sumie M, Sase M, Nakano T, Hara H, et al. Prenatal diagnosis of congenital epulis: a case report. Ultrasound Obstet Gynecol. 2002;20:627-629.
- Kadivar M, Sangsari R, Alavi A. Prenatal diagnosis of granular cell tumor. Iran J Med Sci. 2014;39(2):144-147.
- Wittebole A, Bayet B, Veyckemans F, Gosseye S, Vanwijck R. Congenital epulis of the newborn. Acta Chir Belg. 2003;103:235-237.
- Yuwanati M, Mhaske S, Mhaske A. Congenital granular cell tumor - a rare entity. J Neonatal Surg. 2015;4(2):17.
- Wam Y. Prenatal Sonographic Diagnosis of Congenital Epulis. Journal of Diagnostic Medical Sonography. 2003;19:255-257.
- Sakai VT, Oliveira TM, Silva TC, Moretti AB, Santos CF, Machado MA. Complete spontaneous regression of congenital epulis in a baby by 8 months of age. Int J Paediatr Dent. 2007;17:309-312.