Introduction
Cyclic thrombocytopenia (CTP) is a rare entity with only about a handful of cases worldwide [
1]. It mimics idiopathic thrombocytopenic purpura in its presentation. There are periodic fluctuations in platelet counts with episodes of thrombocytopenia with gradual improvement of platelet counts and at times resulting in rebound thrombocytosis. Tuberculosis has been associated with thrombocytopenia or thrombocytosis. There have been no reports of the same associated with cyclic thrombocytopenia, as was the case in this patient.
Case Report
A 38 year old lady came to the outpatient department with symptoms of easy fatigability and malaise. There had been no symptoms of bleeding, recurrent infection or recent fever. There were no systemic features of loss of appetite or weight. On examination she was found to have an erythematous maculopapular rash of 4 days duration, over the arms and trunk. There was generalized lymphadenopathy, 1x1 cm discrete firm nodes palpable in the submental region and bilateral inguinal regions. The remaining systemic examination was unremarkable.
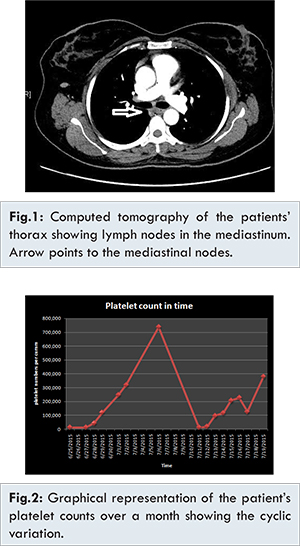
Initial evaluation showed only thrombocytopenia (platelet count of 12,000/cu mm). Her other cell lines were well preserved. Differentials considered at the time were those of lymphoproliferative or myeloproliferative disorders, autoimmune disorders like idiopathic thrombocytopenic purpura (ITP), systemic lupus erythematous (SLE), or CTP. Infectious etiology was considered less likely since there had been no fever. Bone marrow examination was normal. A contrast enhanced computed tomography (CECT) scan of the thorax and abdomen showed multiple borderline nodes, 11 mm maximum [Fig.1]. Her left parailiac node was biopsied which was normal. Multiple markers of myeloproliferative, lymphoproliferative and autoimmune disorders were normal. Her platelet counts were monitored in the ward and she had spontaneous recovery of platelets counts reaching normal values followed by rebound thrombocytosis upto 7 lakh/cu.mm. A week later the platelet counts were again noted to be 12,000/cu mm. Over the period of a week without medical therapy, they gradually improved again to 5 lakh/cu.mm. Thus there had been 2 documented cycles of the same over the period of a month [Fig.2]. She did not have any bleeding manifestations during her hospital stay.
The patient was discharged with a diagnosis of probable idiopathic cyclic thrombocytopenia. Her lymphnode biopsy sample 2 months later grew Mycobacterium tuberculosis on LJ culture. She was then called back and initiated on antituberculous therapy. Since the initiation of the same, she has been asymptomatic with no further cyclic episodes of thrombocytopenia.
Discussion
Cyclic thrombocytopenia is a rare disease often misdiagnosed as idiopathic thrombocytopenic purpura [
2]. There are few other conditions also associated with cyclic thrombocytopenia such as myelodysplastic syndromes and myeloproliferative disorders [
2]. In the absence of these as in our patient, it is diagnosed as idiopathic cyclic thrombocytopenia.
The usual course of the cycle of low platelet to normal platelet is usually 3-5 weeks, but this duration is variable [
3]. In some patients after the period of low platelet count, there may be a rebound thrombocytosis. Many theories have been proposed to explain the cyclic variation. One of these is the variation of the expression of the macrophage Fc receptor to hormonal changes, thus the improvement with danazol in some settings [
4]. Other mechanisms include antiplatelet antibodies whose titers of antiplatelet antibodies vary with variation in platelet count [
5]. Even an infectious cause such as Ehrlichia platys has been identified in dogs [
6].
Tuberculosis is known to cause both thrombocytosis and thrombocytopenia but no cyclic variations have been described to date. Many theories have been proposed to describe the mechanism of thrombocytopenia in tuberculosis. One theory is that of an immune mediated thrombocytopenia - like an idiopathic thrombocytopenic purpura in tuberculosis for the treatment of which immunomodulatory therapy along with anti-tuberculous therapy has been widely used [
7]. It is to be noted that immunomodulatory therapy alone does not improve the same unless concomitant antituberculous therapy is used suggesting a causative role of Mycobacterium tuberculosis. It classically presents in females between the 3rd-8th decade of life of middle eastern or Asian descent. It is associated with pulmonary tuberculosis 33% of the time and with disseminated as well as tuberculous lymphadenitis 19% of the time [
8]. Other theories are those of direct marrow involvement in tuberculosis, drug induced side effects particularly those due to isoniazid to cause marrow suppression, thrombotic thrombocytopenic purpura and DIC. In our patient, a possible immune mediated mechanism is suspected as the cause of thrombocytopenia. She has had no further episodes of the same ever since anti-tuberculous therapy was initiated.
In summary, in the presence of cyclical thrombocytopenia with rebound thrombocytosis, the diagnosis of cyclical thrombocytopenia should be strongly considered. Tuberculosis can rarely cause immune thrombocytopenia. This is the first case report associating cyclic thrombocytopenia with tuberculous lymphadenitis.
References
- Shirota T, Yamamoto H, Fujimoto H, Harada Y, Okada K, Uchida H, et al. Cyclic thrombocytopenia in a patient treated with cyclosporine for refractory idiopathic thrombocytopenic purpura. Am J Hematol. 1997;56(4):272-276.
- Abe Y, Hirase N, Muta K, Okada Y, Kimura T, Umemura T, et al. Adult onset cyclic hematopoiesis in a patient with myelodysplastic syndrome. Int J Hematol. 2000;71(1):40-45.
- Skoog WA, Lawrence JS, Adams WS. A metabolic study of a patient with idiopathic cyclical thrombocytopenic purpura. Blood. 1957;12(9):844-856.
- Rice L, Nichol JL, McMillan R, Roskos LK, Bacile M. Cyclic immune thrombocytopenia responsive to thrombopoietic growth factor therapy. Am J Hematol. 2001;68(3):210-214.
- Yanabu M, Nomura S, Fukuroi T, Kawakatsu T, Kido H, Yamaguchi K, et al. Periodic production of antiplatelet autoantibody directed against GPIIIa in cyclic thrombocytopenia. Acta Haematol. 1993;89(3):155-159.
- Chang AC, Chang WL, Lin CT, Pan MJ, Lee SC. Canine infectious cyclic thrombocytopenia found in Taiwan. J Vet Med Sci Jpn Soc Vet Sci. 1996;58(5):473-476.
- Go RS. Idiopathic cyclic thrombocytopenia. Blood Rev. 2005;19(1):53-59.
- Kalra A, Kalra A, Palaniswamy C, Vikaram N, Khilnani GC, Sood R. Immune thrombocytopenia in a challenging case of disseminated tuberculosis: a case report and review of literature. Case Reports in Medicine. 2010:1-4.