Introduction
One of the most important cardiovascular complications of hypothyroidism is pericardial effusion. The recent review had quoted that the incidence of pericardial effusion among the hypothyroidism patients had ranged between 30% and 75% [1,2]. The distinguishing feature of pericardial effusion caused by hypothyroidism is the absence of sinus tachycardia, which is more common in pericardial effusion caused by other causes [3]. Interventions in the form of pericardiocentesis is usually unnecessary until otherwise there is a significant cardiac tamponade which had developed [4,5]. Echocardiography is the gold standard diagnostic test with a very high sensitivity and specificity in the diagnosis of pericardial effusion [6].
It has been well documented in the literature that the hypothyroidism per se will lead on to concentric left ventricular thickening which would respond gradually to thyroxine therapy [7]. In this context we report a case of primary hypothyroidism presenting with a moderate pericardial effusion.
Case Report
A 60 year old woman got admitted to our hospital with the complaints of chest pain, grade IV dyspnea, swelling of feet, abdominal distension, hoarseness of voice, prominent neck veins and palpitation for past 2 weeks. She also had the history of reduced urine output, loss of appetite and increase in weight. She is a known case of hypothyroidism but had irregular treatment and follow up. Physical examination showed she is obese with a BMI of 31.5, her face was puffy, thyroid gland was enlarged and palpable but it was not tender and there were no nodules on palpation. Bilateral pitting pedal edema was present and the reflexes were pseudomyotonic. Her vitals were as follows, pulse rate: 65/min; blood pressure: 90/60 mm Hg ; respiratory rate: 18/min and heart sounds were found to be distant and muffled.
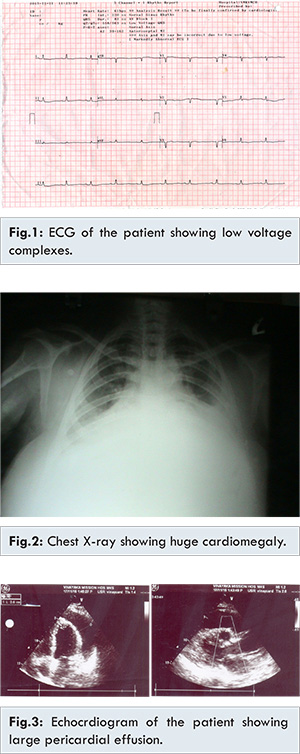
The following blood investigations were conducted on the patient. The complete hemogram showed Hb: 10.9 gm% (N: 12-13 gm%); TLC: 9,100 cells/cu.mm (N: 9,000-11,000); DLC:
P: 66% (N: 60-65%), L: 30% (N: 30-35%), E: 04% (N: 0-5%); ESR : 10 & 20 mm at 30 and 60 mins (N: 5-10 at 30 mins, 10-20 at 60 mins); platelets: 2.01 lakhs/cu.mm (N: 1.5-3 lakhs/cu.mm); bleeding time: 4 mins (N: 2- 4 mins); clotting time : 4.30 min (N: 5-7 mins); urea: 28 mg/dL (N: 20-40 mg/dL); serum creatinine: 0.9 mg/dL (N: 0.7-1.2 mg/dL); serum cholesterol: 200 mg/dL (N: 150-200 mg/dL); triglycerides: 110 mg/dL (N: <150 mg/dL); HD: 47 mg/dL (N: 30-45 mg/dL); LDL: 131 mg/dL (<100 mg/dL); liver function tests : normal study. The thyroid profile of the patient showed - T3: 0.3 pg/mL (N: 1.5 -3.0 pg/ml); T4: 3.15 µg/dL (N: 4-6 µg/dL); TSH: 72.18 mIU/mL (N: 3-5.5 mIU/mL). The ECG of the patient showed low voltage complexes [Fig.1] with a heart rate of heart rate 61/min. Chest X-ray showed huge cardiomegaly [Fig.2] and the two dimensional transthoracic echocardiogram showed large pericardial effusion measuring 22 cm anteriorly and 29 cm posteriorly [Fig.3].
Under the guidance of echocardiography, about 700 ml of pericardial fluid was aspirated through apical approach. The fluid was sent to laboratory for analysis and the report showed were as follows, proteins: 5.6 gm/dL; sugar: 98 mg/dL;
AFB: negative; culture-negative for organisms; microscopy showed few mesothelial cells, cystic macrophages and occasional lymphocytes and degenerated cells. So the fluid was found to be an exudative.
After the fluid aspiration the patient symptoms improved, dyspnoea was reduced. A repeat X-ray had showed the size of the heart had decreased [Fig.4]. The patient was then started with thyroxine 200 µg/day. The patient came for follow up at the end of 1 month and the patient was totally free of symptoms and she is doing well.
Discussion
Hypothyroidism leading on to pericardial effusion is not uncommon but it rarely causes cardiac tamponade. The mechanism of this type of myxedematous pericardial effusion is due to the increased permeability of capillaries and the subsequent leakage of fluid rich in protein into the interstitial space and the impaired lymphatic drainage leading on to salt and water retention [8].
Cardiac tamponade as a complication of hypothyroidism is very rare; Jiménez-Nácher et al. had cited in his study that until 1992 only 27 cases had been described in the world literature. This low incidence is probably due to the slow accumulation of liquid and to cardiac distensibility [7]. Factors described as provoking cardiac tamponade include infection, spontaneous pericardial hemorrhage, non-compliance with thyroid therapy, and abdominal paracentesis. Identification of cardiac tamponade in hypothyroidism is difficult and most of the time it was mistaken for cardiac failure due to its symptoms of tachycardia, rise in venous pressure, lower limb edema, and increased cardiac size on radiography, and all these clinical features were present in our patient.
The primary and the most important phenomenon in cardiac tamponade is the compression of all the four cardiac chambers after the pericardial content reaches the limit of pericardial reserve volume. With smaller cardiac chambers, the myocardial diastolic compliance is reduced and cardiac inflow becomes limited, ultimately equalizing mean diastolic pericardial and chamber pressures. This equalization of pressures is the hallmark of cardiac tamponade [9].
There are certain pathological and hemodynamical changes which were reported in the literature that describes about the hypothyroid heart. The classical pathological examination of a hypothyroid heart reveals a dilated heart with pale and floppy myocardium. Coronary atherosclerosis is quite common in patients with hypothyroidism. Histopathological examination of the myocardium shows interstitial edema and swelling of the muscle fibers with loss of striations, which is a hallmark of myocardial muscle. The pericardial sac usually contains fluid rich in protein and mucopolysaccharides [10]. In our study, patient also we had the pericardial fluid analysis showing rich in proteins.
Reversible echocardiographic abnormalities are usually documented in a hypothyroid heart. Heart dilatation, reduced myocardial contractility, enlarged thickness of the interventricular septum and increase in the left ventricular volume had been described in the earlier studies [10] and in our study also the patients echocardiography picture had shown left ventricular hypertrophy and the dilatation of heart. This state usually mimics hypertrophic and dilated cardiomyopathies, but these abnormalities can be reversed by bringing the hypothyroid state to normal [11]. It is well documented in the literature that the hypothyroidism can per se lead on to concentric left ventricular thickening that responds to gradually to thyroxine therapy [12].
The main stay in the treatment for the hypothyroid causing pericardial effusion is simple thyroxine replacement, but in few exceptional cases where the patient is presenting with a tamponade mandates urgent pericardiocentesis, in our study also pericardiocentesis was performed on the patient and about 700 ml of pericardial fluid was aspirated and patient had become asymptomatic.
The clinical resolution of pericardial effusion is satisfactory in majority of the hypothyroid patients with thyroxine replacement therapy, but it takes as long as months or years after the patient reach the euthyroid state [13]. In our patient, at the end of one month follow up her thyroid status was brought to almost near normal and she had no symptoms related to cardiovascular system.
Conclusion
Hypothyroidism at times has rare modes of presentation and on many occasions it might go unrecognised. Hypothyroidism should be ruled out as an underlying cause of pericardial effusion especially in the middle aged females. The treatment is simple and gratifying, where majority of the patients with mild effusion will get settled with thyroxine therapy alone and only patients with tamponade might need pericardiocentesis.
References
- Hardisty CA, Naik DR, Munro DS. Pericardial effusion in hypothyroidism. Clin Endocrinol. 1980;13:349-354.
- Kerber RE, Sheman B. Echocardiographic evaluation of pericardial effusion in myxedema. Incidence and biochemical and clinical correlations. Circulation. 1975;52:823-827.
- Kabadi UM, Kumar SP. Pericardial effusion in primary hypothyroidism. Am Heart J. 1990;120:1393-1395.
- Ingbar SH, Larsen PR. The thyroid gland. In: Wilson JD, Foster DW, eds. Williams textbook of endocrinology. Philadelphia: WB Saunders;1992:357-487.
- Motabar A, Anousheh R, Shaker R, Pai RG. A rare case of amiodaroneinduced hypothyroidism presenting with cardiac tamponade. Int J Angiol. 2011;20:177-180.
- Calvo-Elipe A, Monoz-ruiz AI, Cano-Ballesteros JC. Cardiac tamponade in a woman with primary hypothyroidism. Ann Med Intern. 1995;12:503-504.
- Jimenez-Nacher JJ, de-Alonso N, Vega B. Cardiac tamponade as a presentation of primary hypothyroidism in a young woman. Rev Clin Esp. 1993;193:290-292.
- Hayat Al Mahroos, Rashid Al Bannay. Massive Pericardial Effusion as a sole Manifestation of Hypothyroidism - A Case Report. Bahrain Medical Bulletin. 2000. Vol.22, No.4.
- Rachid A, Caum LC, Trentini AP, Fischer CA, Antonelli DAJ, Hagemann RP. Pericardial Effusion with Cardiac Tamponade as a Form of Presentation of Primary Hypothyroidism. Arq Bras Cardiol. 2002;78(6):583-585.
- Sinha A, Hyndavi Yeruva SL, Kumar R, Curry BH. Early Cardiac Tamponade in a Patient with Postsurgical Hypothyroidism. Case Reports in Cardiology Volume 2015 (2015). http://dx.doi.org/10.1155/2015/310350.
- Fazio S, Palmieri EA, Lombardi G. Effects of thyroid hormone on cardiovascular system. Re-cent Progress in Hormone Research. 2004;59:31-50.
- Dernellis J, Panaretou M. Effects of thyroid replacement therapy on arterial blood pressure in patients with hypertension and hypothyroidism. American Heart Journal. 2002;143:718-724.
- Patil VC, Patil HV, Agrawal V, Patil S. Cardiac tamponade in a patient with primary hypothyroidism. Indian J Endocrinol Metab. 2011;15(Suppl2): S144-S146.