|
|
|
|
|
Cortical Venous Thrombosis due to Familial AT-III Deficiency Presenting with Seizures
|
|
|
Swastik Purkait1, Kaushik Ghosh2, Jaydeep Samanta1, Sanat Kumar Jatua1, Ambarish Bhattacharya3, Manas Ghosh2
Department of Medicine, 1NRS Medical College & Hospital, Kolkata; 2Murshidabad Medical College, Berhampore; 3Charnok Hospital, Kolkata, West Bengal, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Kaushik Ghosh
Email: drkaushikghosh@gmail.com
|
|
|
|
|
|
|
|
|
Received:
24-DEC-2015 |
Accepted:
22-MAR-2016 |
Published Online:
05-MAY-2016 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Cortical venous thrombosis is a rare but treatable condition of the central nervous system which can manifest with bizarre signs and symptoms. However, a prompt clinical suspicion which can be confirmed by a T2 weighted MR image followed by venography is immediately needed to assess the patient and start therapy. We report a case of familial anti-thrombin III deficiency in a young male who presented to us with seizures.Successful treatment of this patient holds promise of an essentially non curable neurological condition. |
|
|
|
|
|
Keywords :
|
Antithrombin-III deficiency, Humans, Seizures, Thrombin, Venous Thrombosis.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff449f0c000000ab04000001001100 6go6ckt5b5idvals|604 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Cortical venous thrombosis is presence of thrombosis in dural venous sinuses. It is rare condition with an estimated annual incidence of 3-4 cases per million in adults [1]. Although it is a serious condition still it is potentially treatable with standard anticoagulation. Superior sagittal sinus is most commonly affected and females of reproductive age groups are commonly affected. Headache due to increased intracranial pressure is the most commonly reported symptom followed by focal neurological deficit [2]. Bizarre combination of focal or global neurological deficits not explained by vascular territory along with history of predisposing factors is the key note of diagnosis. With advent of newer diagnostic technology like magnetic resonance imaging and venography, it is more often diagnosed than a couple of decades ago. Still clinical suspicion is the corner stone for reaching the diagnosis. Here we present a case of 16 year old male who presented to us with repeated episodes of seizures and was found to have cortical venous thrombosis and was successfully treated with anticoagulants. Subsequently investigations showed that he has hereditary antithrombin III deficiency.
Case Report
A 16 year old male presented to us with history of repeated episode of generalized tonic clonic seizures for 3 days. There was no prior history of seizure disorder. He is not hypertensive or diabetic and denies any kind of substance abuse. There is no history of fever or working in extreme heat or any trauma. On examination, patient was drowsy with a GCS of 12/15 (E4V4M4). There was no focal neurological deficit except plantars being not elicitable bilaterally. At presentation his blood pressure was 110/66 mm of Hg, pulse 88/min, temperature 97.8oF. However, fundoscopy showed mild blurring of disc margins more on left side.Examination of abdomen, respiratory system, cardiovascular system was normal. His initial investigations are mentioned in Table 1.
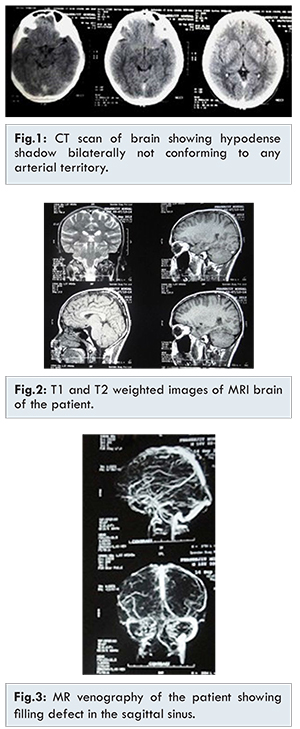
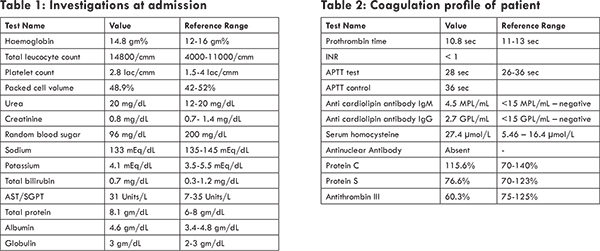
Empirically phenytoin sodium and lorazepam were intravenously started to control the seizure and computer tomography(CT) of brain was requested. CT head showed hypodense non-enhancing lesion in the upper posterior part of the left temporal and adjacent parietal lobe and in sagittal sinus without mass effect [Fig.1]. With suspicion of cortical venous thrombosis, coagulation profile [Table 2] and magnetic resonance imaging and venography [Fig.2,3] were performed. From these imaging studies, diagnosis of cortical venous thrombosis was confirmed and anticoagulants were started.Pro-coagulant screen was performed [Table 2]. His antithrombin III level was reported as 60% which was far lower than the referral normal range. We undertook a family screening. As the only living first degree relative was his mother we also sent her blood sample for coagulation screen. His mother’s antithrombin III level was reported as 51.5%. He planned for genetic assay but this was beyond the scope of our institutes and the patient did not consent for this expensive test.
He was immediately started on injection enoxaparin 60 mg subcutaneously twice daily and after 3 days was also started on tablet warfarin. Both drugs were overlapped for 3 days and then only warfarin was continued. Warfarin was titrated to keep an INR of 2.5 to 3. His mother was also admitted and started on the same treatment.
Currently he is asymptomatic and is on regular follow-up.
Discussion
Cortical venous thrombosis is the presence of thrombus in the dural venous sinus/sinuses. Bizarre combination of focal or global neurological deficits not explained by a definite vascular territory along with history of predisposing factors is the key to reaching this diagnosis. With the advent of newer diagnostic technology like magnetic resonance (MR) imaging and MR venography, it has been diagnosed more in the last couple of decades. Still clinical suspicion is the corner stone for reaching the diagnosis. Here we present a case of an 18 years old male who presented to us with repeated episodes of seizures and was found to have cortical venous thrombosis and was detected and successfully treated with anticoagulants. Subsequently investigations showed that he has hereditary antithrombin III deficiency.
Antithrombin is a plasma protease inhibitor that neutralizes thrombin and factors Xa, IXa, and XIa by irreversibly forming 1:1 complexes in reactions accelerated by heparin or by heparin sulphate on endothelial surfaces [1]. Therefore, defects in antithrombin, compromise the normal inhibition of the coagulation pathways and cause a hypercoagulable state [1]. Cortical venous sinus thrombosis is found mostly in females (almost 75%) and has been commonly associated with hypercoaguable states like pregnancy, oral contraceptives and malignancies [2]. There are only very few case of cortical venous thrombosis due to antithrombin III deficiency reported in literature till date. Even though males are affected much lesser than females it becomes even more important as male sex has been identified as a bad prognostic marker in cases of cortical venous thrombosis [2].
Antithrombin deficiency can be either hereditary or acquired. Hereditary deficiency is also a heterogeneous disorder which is generally inherited as an autosomal dominant manner. Although most cases are familial new onset mutation causing antithrombin deficiency has also been reported [3]. Hereditary antithrombin deficiency can be of two types [4]: Type I is caused as a result of reduced synthesis while type II isdue to molecular defect within the protein so that it does not function properly. Generally, in type I defect antithrombin activity is between 40-60% and in most cases of Type II defect antithrombin activity is between 60%-80% [4]. However, a Type III has also been reported where the molecule is structurally and functionally normal but somehow there is improper interaction between the AT and heparin [5]. Acquired antithrombin deficiency can occur due medication with heparin, disseminated intravascular coagulation, liver disease or nephrotic syndrome [6,7].
The mainstay of treatment in AT-III deficiency is symptomatic, antithrombotic therapy and AT concentrate [8]. Sadly AT concentrate is not widely available in India as yet. However, we should aim to re-canalize the occluded sinus or vein as far as possible so as to return the patient to normalcy as far as possible, in addition to prevention of propagation of the thrombus. Anticoagulation in the form of antithrombotic therapy also prevents the formation of thrombus at other sites in the body, such as pulmonary or renal vasculature and their resultant adverse effects.
Conclusion
Cortical venous thrombosis is commonly overlooked vascular event with varied neurological manifestations. High clinical suspicion of predisposing factors which may attribute to this condition and neurological manifestations beyond presentation of vascular territories is the hallmark of diagnosis. Among various causes of cortical venous thrombosis, AT-III deficiency is a rare but treatable entity. Successful outcome of such patients depends upon prompt clinical acumen, neuroimaging confirmation and early treatment preferably with AT concentrates or standard available anticoagulants.
References
- Stam J. Thrombosis of the Cerebral Veins and Sinuses. New England Journal of Medicine. 2005;352(17):1791-1798.
- Ferro, J, Canhão, P, Stam, J, Bousser, M, Barinagarrementeria F. Prognosis of Cerebral Vein and Dural Sinus Thrombosis Results of the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT). Stroke. 2004;35(3):664-670.
- Muramatsu S, Mizuno Y, Murayama H, Ikemoto S. Hereditary antithrombin III deficiency with a superior sagittal sinus thrombosis: Evidence for a possible mutation starting in the mother of the propositus. Thrombosis Research. 1990;57(4):593-600.
- Kristin Jochmans, Willy Lissens, Ting Yin, Jan Jacques Michiels, Leonie van der Luit, et al. Molecular Basis for Type 1 antithrombin Deficiency: Identification of Two Novel Point Mutations and Evidence for a De Novo Splice Site Mutation. Blood. 1994;84(11):3742-374.
- Tait RC, Walker ID, Perry DJ, Islam SI, Daly ME, McCall F, et al. Prevalence of antithrombin deficiency in the healthy population. Br J Haematol. 1994;87:106-112
- Von Kaulla K, Ens G. On structure-related properties of synthetic organic clot-dissolving (thrombolytic) compounds. Biochemical Pharmacology. 1967;16(6):1023-1034.
- Kauffmann R, Veltkamp J, Van Tilburg N, Van Es L. Acquired antithrombin III deficiency and thrombosis in the nephrotic syndrome. The American Journal of Medicine. 1978;65(4):607-613.
- Jarial D. Cerebral Venous Thrombosis due to Antithrombin III Deficiency in Adolescent. Pediatric Oncall. 2013;10(4).
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Purkait S, Ghosh K, Samanta J, Jatua SK, Bhattacharya A, Ghosh MCortical Venous Thrombosis due to Familial AT-III Deficiency Presenting with Seizures.JCR 2016;6:195-198 |
|
Purkait S, Ghosh K, Samanta J, Jatua SK, Bhattacharya A, Ghosh MCortical Venous Thrombosis due to Familial AT-III Deficiency Presenting with Seizures.JCR [serial online] 2016[cited 2026 Jun 29];6:195-198. Available from: https://www.casereports.in/articles/6/2/Cortical-Venous-Thrombosis-due-to-Familial-AT-III-Deficiency-Presenting-with-Seizures.html |

|
|
|
|
|