|
|
|
|
|
Double Segmental Tibial Fracture: Case Report with Review of Literature
|
|
|
Dhananjay Singh, Bhanu Awasthi, Vikas Padha, Vivek Negi
Department of Orthopaedics, Dr RPGMC, Tanda, Kangra, Himachal Pradesh, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Dhananjay Singh
Email: chocoedbe3@gmail.com
|
|
|
|
|
|
|
|
|
Received:
11-FEB-2016 |
Accepted:
26-APR-2016 |
Published Online:
05-JUN-2016 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
We report a 51 year old male with open double segmental fracture of both bones of left leg after being allegedly hit by a car. Patient was initially treated by toileting, debridement and nailing, followed by bone grafting at a later date. Segmental tibial fractures are uncommon and double segmental fractures/trifocal fractures are rarely seen, literature search revealed that only three such cases and only one treated previously by intramedullary nail. Intramedullary nail remains effective treatment modality of such fractures and these fractures often require bone grafting. |
|
|
|
|
|
Keywords :
|
Bone Transplantation, Fracture Fixation, Fractures, Leg, Tibial Fractures.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff843b0d000000ba04000001000f00 6go6ckt5b5idvals|616 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Segmental tibial fractures are an uncommon injury pattern accompanied by significant soft tissue trauma and higher complication rates. Various modalities of treatment have been described for such fracture patterns [1]. We report a very rare injury pattern of a double segmental/ three level bone fracture pattern treated with intramedullary nailing.
Case Report
A 51 year old chronic smoker and alcoholic patient reported in the casualty following a roadside accident after being allegedly hit by a car. He presented with deformity and bleeding from the left leg. There was a wound of size 0.5 centimeters present on the distal one-third of the left leg with two deep abrasions, one over medial malleolus and one over mid-leg [Fig.1]. X-rays revealed a double segmental/ three level fracture of tibia and fibula [Fig.1,2]. Patient’s limb was immobilized in an above knee slab after thorough wound wash and intravenous antibiotics were started. Patient was posted for surgery next day.

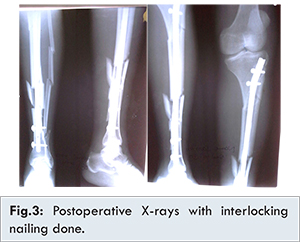
Patient was planned for debridement, toileting and fixation with interlocking nail tibia. Due to non-availability of C-arm due to technical reasons, cannulated nail of smallest available diameter was used for fracture fixation. Entry point was kept more lateral than usual. Guide-wire was negotiated carefully sequentially across the fractures while manually holding the reduction using anterior border of tibia as reference. Distal most fracture was open so wound was extended for toileting and guide-wire was negotiated under direct vision through distal most fracture. Smallest available cannulated nail of 8 millimeters size was passed over guide-wire. Distal locking was done free hand using technique described by Soni and Mehta et al. [2]. Proximally two bolts were inserted with jig [Fig.3]. The distal most segment developed vertical split while negotiating the nail but soft tissue attachments of split fragments were carefully preserved. Post-operative wound healing was uneventful and patient was discharged with strict instructions to quit smoking and alcohol.
Patient came for first follow-up at three months with proximal most fracture showing union and distal most fracture showing no evidence of union. Patient was advised admission for bone grafting but was lost to follow-up. Bone grafting was performed six months following first surgery. Distal most fracture site was opened, and sclerotic fracture ends were freshened till bleeding was visible. Cortico-cancellous bone graft was harvested from ipsilateral iliac crest and placed at the fracture site and wound closed on negative suction drain. Post-operative period was uneventful. After nine months of initial trauma, all fractures showed evidence of union [Fig.4] with painless weight-bearing without any fresh complaints and good limb alignment and function.
Discussion
Segmental tibia fractures are uncommon fracture patterns caused by high energy trauma. Half of them are open with severe soft tissue injury [3]. According to Giannoundis, two thirds need more than one surgical procedure [4]. Blind nailing, as in our case was described way back in 1969 by Zucman and Maurer [5].
A thorough search using keywords double segmental tibia fractures and three level tibia fractures reported only three cases with this very rare pattern - one managed conservatively [6], one using expert tibia nail with primary bone grafting [7] and one using three locking compression plates [8]. Sarmiento et al. managed a double segmental tibial fracture using functional treatment [6]. No attempt was made to regain length. The fracture healed with the same initial shortening and with good alignment. We went for operative treatment as our case had open fracture. Bali et al. managed open double segmental tibial fracture using expert tibial nail [7]. They waited for ten days before definitive treatment and performed primary bone grafting. We performed definite fixation on next day of presentation and bone grafting was performed at a later date. Garcia et al. managed a case using three locking compression plates [8]. Their case had intraarticular fractures of proximal and distal tibia with midshaft fracture of tibia. Our case had all fractures in the tibial shaft. Only a limited number of studies are available for management of segmental tibia fractures [3,4,5]. Various modalities of treatment include intramedullary nailing, long plates, external fixators and conservative management by some. Giannoudis et al. achieved a deep infection and malunion rate of 50% when treating eight segmental tibia fractures with external fixation [4] which discouraged us from using this mode of treatment. Intra-medullary nail offers the advantage of preserving vascularity, surgical incisions away from fracture sites along with early weight bearing making it an ideal implant for such fracture patterns.
Conclusion
Intramedullary nailing is an effective means of treatment of segmental tibia fracture as it avoids excessive soft tissue stripping and early mobilization. In our case we used cannulated interlocking nail but careful attention to entry point, alignment and soft tissue attachments led to good outcome in our patient, even though there was a vertical split of the third distal fragment and union was achieved following bone grafting.
References
- Mcmurtry J, Mounasamy V. Segmental tibia Fractures. Annals of Orthopedics & Rheumatology. 2015;3(3):1051.
- Soni RK, Mehta SM, Awasthi B, Singh JL, Kumar A, Thakur L, et al. Radiation-free Insertion of Distal Interlocking Screw in Tibial and Femur Nailing: A Simple Technique. Journal of Surgical Technique and Case Report. 01/2012;4(1):15-18.
- Woll TS1, Duwelius PJ. The segmental tibial fracture. Clin Orthop Relat Res. 1992;(281):204-207.
- Giannoudis PV, Hinsche AF, Cohen A, Macdonald DA, Matthews SJ, Smith RM. Segmental tibial fractures: an assessment of procedures in 27 cases. Injury. 2003; 34(10):756-762.
- Zucman J, Maurer P. Two-level fractures of the tibia. Results in thirty-six cases treated by blind nailing J Bone Joint Surg Br. 1969;51(4):686-693.
- Sarmiento A, Latta LL. In: The Nonsurgical Treatment of Fractures in Contemporary Orthopedics, 1st edition. Mc Graw Hill Education, 2011.
- Bali K, Kumar V, Patel S, Aggarwal S. Double segmental tibial fractures-an unusual fracture pattern. Chinese Journal of Traumatology, Zhonghua Chuang Shang za Zhi. 2011;14(4):247-249.
- Garcia AF, Ashford RU, DeBoer PG. Three-level tibial fracture treated by minimally invasive techniques. Injury Extra. 2006;37:60-63.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Singh D, Awasthi B, Padha V, Negi VDouble Segmental Tibial Fracture: Case Report with Review of Literature.JCR 2016;6:243-246 |
|
Singh D, Awasthi B, Padha V, Negi VDouble Segmental Tibial Fracture: Case Report with Review of Literature.JCR [serial online] 2016[cited 2026 May 21];6:243-246. Available from: http://www.casereports.in/articles/6/2/Double-Segmental-Tibial-Fracture.html |

|
|
|
|
|