|
|
|
|
|
Giant Lipoma of Parotid Gland
|
|
|
Bharat Gupta, Gurbinder Singh, Vikas Garg, Mayur Vira, Sohan Singh
Department of Radiodiagnosis & Imaging, Government Medical College & Hospital Amritsar 143001, Punjab, India.
|
|
|
|
|
|
Corresponding Author:
|
Dr. Bharat Gupta
Email: bharatgupta3009@gmail.com
|
|
|
|
|
|
|
|
|
Received:
29-JAN-2015 |
Accepted:
08-MAR-2016 |
Published Online:
05-APR-2016 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Lipomas are common soft tissue neoplasms. They are rarely seen in parotid gland, often not considered in the initial differential diagnosis of parotid gland tumors. Lipomas account for 0.6% to 4.4% of all parotid tumors. Superficial lobe is common site of origin in parotid gland with only rare reports from deep lobe. When there is any suspicion, imaging studies are of high diagnostic value. We present a case of parotid lipoma involving the deep and superficial lobes of the parotid gland. Computed tomography (CT) and ultrasound were performed in radiological diagnosis. Findings were confirmed by fine needle aspiration cytology. |
|
|
|
|
|
Keywords :
|
Biopsy, Diagnosis, Lipoma, Parotid Gland, Parotid Neoplasms.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff44220c0000008d04000001000f00 6go6ckt5b5idvals|591 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Lipoma is common benign mesenchymal tumor usually seen in fatty areas of body [1]. Rarely are lipomas seen in head & neck region [1-4]. In the head and neck, it arises mainly in the posterior cervical triangle and forehead. On rare occasions, however, it may occur in the pharynx, larynx, especially oral cavity, parotid gland and parapharyngeal space [1,3,5-7]. The lipoma of parotid gland is a rare entity, comprising 0.6%-4.4% of all parotid tumors in the literature, with most series reporting an incidence of 1%-2% of all parotid tumors and 2.6% of benign tumors [1,3,8]. Lipomas arising from deep lobe of parotid gland are even rarer with only few cases reported in literature [9]. CT and MRI are diagnostic with aspiration cytology increasing the diagnostic confidence. Surgical intervention in these tumors is challenging because of the proximity of the facial nerve [9].
Case Report
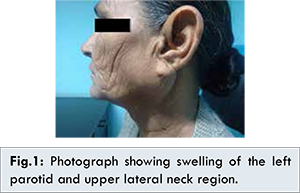
A 55 year old female was referred to our radiology department for CT scan of the face and neck for a visible painless swelling in the left parotid region [Fig.1]. She noticed the swelling 2 years back and was progressively increasing since then. On examination the parotid swelling was elastic, soft, mobile, non-tender and non-fluctuant. Overlying skin was normal and there was no associated swelling in the head and neck region.
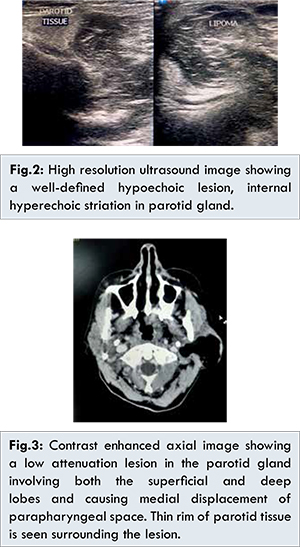
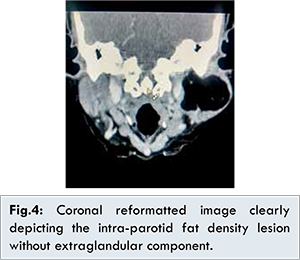
On high frequency ultrasound a well defined encapsulated lesion was seen in the left parotid gland involving the superficial and deep lobe of the gland [Fig.2]. Lesion was hypoechoic as compared to the normal gland parenchyma. Linear hyperechoic strands with no calcification or cystic area or vascularity was noted. Contrast enhanced CT scan was performed on a MDCT starting from base of skull upto supraclavicular region with sagittal and coronal reformatting. Contrast enhanced CT scan showed a well marginated fat density (-100 HU) lesion in the substance of left parotid gland involving both superficial and deep lobes with bulk of the lesion in the superficial lobe. Thin rim of parotid tissue was seen at the periphery. Left parapharyngeal space was displaced medially. No enhancing soft tissue component was visualized in the lesion [Fig.3,4].
Fine needle aspiration cytology was performed which supported the diagnosis of lipoma. Patient was referred to the department of head & neck surgery for further management [Fig.5].
Discussion
Lipomas of the salivary gland are rare entities with highest frequency reported in parotid gland [4]. They are the most commonly encountered benign mesenchymal tumors that are histologically similar to mature adipose tissue, but the presence of a fibrous capsule helps to differentiate them from simple fat aggregations [10]. Lipoma of the parotid gland are extremely rare with lipomas arising from deep lobe of parotid gland even rarer [9]. Different causes of lipomas are mentioned in the literature: heredity, obesity, diabetes, radiation, endocrine disorders, insulin injection, corticosteroid therapy and trauma [3]. In general incidence of parotid lipoma is much more common in males with male: female ratio of 5:1 [11]. Ultrasound screening showing a homogenous hypoechoic lesion can give a quick diagnosis [8].
CT shows a hypodense and homogeneous mass with uniform fat density throughout [3]. The normal parotid tissue reveals positive density, whereas lipomatous tissue will give negative attenuation (-50 to -150 Hounsfield units) [4,12]. CT scan sometimes does not differentiate between normal parotid gland and lipomatous tissue. This information can be clearly obtained from MRI scan, which thus becomes the ideal radiological investigation for such tumors [4]. The normal parotid gland has a high fat content and is easily visualized on both CT and MRI, and therefore both techniques can demonstrate whether a mass in that region is intraglandular or extraglandular [13]. MRI presents the typical signal intensity patterns with high signal intensity on T1- and T2-weighted images. No enhancement is seen on post-contrast images, fat suppressed sequences are specific in diagnosis showing signal loss. MRI can also clearly define the limits of lipoma from normal adipose tissue (subcutaneous tissue) with a “black-rim” around the mass, a distinction that cannot be made from CT [1,3,8]. Moreover, MRI is sufficiently accurate to distinguish between lipomas and liposarcomas. Although MRI may prove to be a better diagnostic tool regarding tumor margin characteristics, has no added benefit in changing management strategy. CT and/or MRI scans are more reliable than FNA cytology in accurate diagnosis of parotid lipomas. FNA cytology are supportive in diagnosis of lipomatous lesions and should be considered if there is any suspicion of malignancy [14].
Conclusion
Lipoma of the parotid gland involving the deep and superficial lobe is a rare entity. Diagnosis can be made with confidence on imaging including ultrasound, CT, MRI as diagnostic modalities of choice.
References
- Debnath SC, Saikia, A. Lipoma of the Parotid Gland Extending from the Superficial to the Deep Lobe: A Rarity. British Journal of Oral and Maxillofacial Surgery. 2010; 48:203-204.
- Khorsandi Ashtiani MT, Yazdani N, Saeedi M, Amali A. Large Lipoma of the Larynx: A Case Report. Acta Medica Iranica. 2010;48:353-356.
- Dispenza F, De Stefano A, Romano G, Mazzoni A. Post-Traumatic Lipoma of the Parotid Gland: Case Report. Acta Otorhinolaryngologica Italic. 2008;28:87-88.
- Chakravarti A, Dhawan R, Shashidhar TB, Shakuntala, Sahni JK. Lipoma of the Deep Lobe of Parotid Gland-A Case Report and Review of Literature. Indian Journal of Otolaryngology and Head Neck Surgery. 2008;60:194-196.
- Kimura Y, Ishikawa N, Goutsu K, Kitamura K, Kischimoto S. Lipoma in the Deep Lobe of the Parotid Gland: A Case Report. Auris Nasus Larynx. 2002;29:391-393.
- RK A, PN N, S Y, VK A, KK D. Intraoral Lipoma: A Rare Case Report and Review of Literature. Journal of Clinical and Diagnostic Research. 2013;7:3090-3091.
- Nader S, Nikakhlagh S, Rahim F, Fatehizade, P. Endolaryngeal Lipoma: Case Report and Literature Review. Ear, Nose Throat Journal. 2012;91: E18-E21.
- Fakhry N, Justin M, Varoquaux A, Antonini, F, Santini L, Lagier A, et al. Is Surgical Excision of Lipomas Arising from the Parotid Gland Systematically Required? European Archives of Oto-Rhino-Laryngology. 2012;269:1839-1844.
- Wu CW, Chi HP, Hsu YC, Chan LP, Kuo WR. Giant lipoma arising from the deep lobe of parotid gland. World J Surg Oncol. 2006;4:28.
- Kim YH, Reiner L. Ultrastructure of lipoma. Cancer 1982;50(1):102-106.
- El Monem MH, Gaafar AH, Magdy EA. Lipomas of the Head and Neck: Presentation Variability and Diagnostic Workup. The Journal of Laryngology Otology. 2006;120:47-55.
- Cummings CW. Cummings Otolaryngology: Head & Neck Surgery. Vol. 2, Chapter 60: Benign Neoplasms of the Salivary Glands. 4th Edition, Elsevier Mosby, 2005.
- Korentager R, Noyek AM, Chapnik JS, et al. Lipoma and Liposarcoma of the Parotid Gland: High Resolution Preoperative Imaging Diagnosis. Laringoscope. 1988;98:967-971.
- Layfield LJ, Glasgow BJ, Goldstein N, Lufkin R. Lipomatous lesion of the parotid gland: potential pitfalls in fine needle aspiration biopsy diagnosis. Acta Cytol. 1991;35:553-556.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Gupta B, Singh G, Garg V, Vira M, Singh SGiant Lipoma of Parotid Gland.JCR 2016;6:145-148 |
|
Gupta B, Singh G, Garg V, Vira M, Singh SGiant Lipoma of Parotid Gland.JCR [serial online] 2016[cited 2026 May 21];6:145-148. Available from: http://www.casereports.in/articles/6/2/Giant-Lipoma-of-Parotid-Gland.html |

|
|
|
|
|