Introduction
Myxofibrosarcoma is one of the most common sarcomas seen in adult extremities. This neoplasm is particularly seen in elderly patients. It may also arise in the head and neck region. Growth in nodular pattern is the distinctive feature seen under the microscope. By microscopic examination based on number and appearance of cells, myxofibrosarcoma can be divided into low-grade and high-grade. Wide surgical excision of the primary lesion in conjunction with radiation therapy is the treatment of choice for most patients with this tumor. The follow-up of myxofibrosarcomas patients is fundamental to detect local recurrences or early distant metastasis [
1].
Case Report
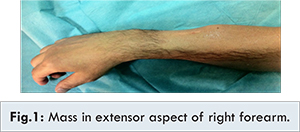
A 46 year old man, without medical or surgical antecedents, and without personal or family history of malignancy or traumatism, was admitted to our institution for a non-tender right forearm mass which evolved during last two months. Physical examination revealed a 5x3 cm firm, non-tender and fixed mass in the extensor aspect of right forearm located distally [Fig.1]. The wrist flexion was difficult. The axillary lymphatic nodes were not palpable.
The patient was screened for metastases using computed tomography. No lesions were seen on scans of the lung or abdomen. Bone scintigraphy was normal. Other routine tests, including plasma biochemistry, liver function tests and urinalysis were normal. MRI of forearm showed a mass in extensor aspect of right forearm located distally, enhancing after injection of gadolinium measuring 28x34 mm and a height of 5 cm in intermusculaire topography, this process was in intimate contact with the deep vascular pedicle of the posterior muscle lodge [Fig.2]. These imaging findings suggested that the mass was neoplastic. Tissue biopsy was performed, and histopathological examination reported that the tumor was predominantly composed of a large number of diffuse fusiform cells in a loose bottom. In addition, mitoses [Fig.3] and presence of fusiform cells in myxoid matrix was seen [Fig.4]. The tumor cells had elongated nuclei and granular chromatin anisokaryosis. The PS 100 [Fig.5] and the SMA (smooth muscle actin) were positive in immunochemistry [Fig.6]. These cytological findings suggested a high grade of a myxofibrosarcoma. The patient underwent operation for tumor resection. The incision was centered on the posterior tumor of the scar allowing excision of the entire skin and deep path of the biopsy [Fig.7].
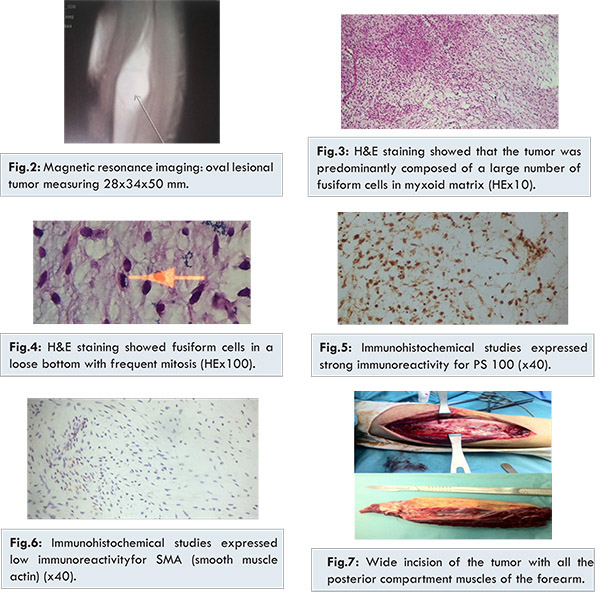
We performed a wide excision of the tumor block with a margin of healthy tissue over its entire surface without seeing the tumor during dissection and we performed a removal of all the posterior compartment muscles of the forearm with safety margin of 5 cm each side of the tumor. The surgical margin was microscopically free of tumor. A volar splint was established for 45 days. Reeducation sessions following the surgery were realized and the recovery of wrist extension and fingers function was satisfactory.
Macroscopically, the excised specimen was a white myxoid mass measured 5x4x4 cm. On the cut section, fusiform cells with central necrosis and frequent mitosis were observed. Microscopic features were identical to that of the biopsy. Immunohistochemical studies showed that the tumor cells expressed strong immunoreactivity for PS 100, low expression of cluster of differentiation 34 (CD 34) and SMA. The combination of clinical and pathological features revealed high-grade myxofibrosarcoma. The patient received postoperative adjuvant radiation after 6 cycles of chemotherapy with doxorubicin, ifosfamid and holoxan every 15 days. There was no evidence of metastasis or local recurrence on one year follow up.
Discussion
Myxofibrosarcoma is a myxoid variant of malignant fibrous histiocytoma (MFH) that most commonly involves dermal and subcutaneous tissues in the extremities of elderly people [
2-
4]. In 1996, Mentzel et al. [
4] reported 75 cases of myxofibrosarcomas and divided these tumors into 3 categories: low, intermediate, and high-grade, depending on the degree of cytologic atypia and the presence or absence of pleomorphic MFH-like lesion within the tumor.
Different clinical studies of myxofibrosarcomas showed that 77% of the tumors occurred in the extremities and about 12% in the trunk, with a high incidence in the dermal or subcutaneous tissues [
2-
4]. Other sites for myxofibrosarcomas reported in the literature include head and neck region, pelvis, retroperitoneum or mediastinum (8%), and heart [
4,
5]. However, a primary myxofibrosarcoma with bone invasion was rarely reported [
6,
7]. In addition, the peak age incidence of myxofibrosarcomas was in the fifth to seventh decades with a male predominance [
3,
8]. The etiology of this malignant tumor remains unknown [
9].
Distinctive histological features of myofibrosarcoma are nodular growth pattern; a myxoid matrix containing elongated, curvilinear capillaries and fusiform, round or stellate tumor cells with indistinct cell margins, slightly eosinophilic cytoplasm, and hyperchromatic atypical nuclei [
4]. In view of strong propensity for intermediate and high grade MFS to develop local recurrences, about half of which are multiple, we feel that initial aggressive local therapy is imperative. Furthermore, probability of limb preservation increases with prevention of local recurrence. We believe that surgery should be performed with a goal of attaining greater than 1 cm resection margins whenever it is possible and that radiotherapy should be considered for all patients diagnosed with high grade MFS.
Future studies should address strategies to intensify local treatment, such as radiation dose escalation and the potential role of radiation sensitizers and/or systemic chemotherapy [
10].
Conclusion
Myxofibrosarcoma is a mesenchymal tumor with a poor prognosis. Extensive surgical excision with adjuvant radiotherapy presents the optimal therapeutic option. The management of this tumor must include multidisciplinary approach consisting of pathologists, traumatologics, radiotherapeutics and oncologists.
Acknowledgements
We thank Mr OUKABLI Mohamed, Department of Pathology, Military Hospital MOHAMED V, Rabat, Morocco, for helping in pathological diagnosis.
References
- Fukunaga M, Fukunaga N. Low-grade myxofibrosarcoma: progression in recurrence. Pathol Int. 1997;47(2-3):161-165
- Angervall L, Kindblom LG, Merck C. Myxofibrosarcoma. A study of 30 cases. Acta Pathol Microbiol Scand A. 1977;85A(2):127-140.
- Weiss SW, Enzinger FM. Myxoid variant of malignant fibrous histiocytoma. Cancer. 1977;39(4):1672-1685.
- Mentzel T, Calonje E, Wadden C, Camplejohn RS, Beham A, Smith MA, et al. Myxofibrosarcoma. Clinicopathologic analysis of 75 cases with emphasis on the low-grade variant. Am J Surg Pathol. 1996;20(4):391-405.
- Wang JG, Li YJ, Liu H, Zhao P. Primary cardiac myxofibrosarcoma: a case report and review of the literature. Tumori. 2012;98(6):e165-e168.
- Kapur P, Sarode V. Pathologic quiz case: myxoid tibial lesion in a 31-year-old man. Low-grade myxofibrosarcoma. Arch Pathol Lab Med. 2004;128(4):e65-e66.
- Park SW, Kim HJ, Lee JH, Ko YH. Malignant fibrous histiocytoma of the head and neck: CT and MR imaging findings. Am J Neuroradiol. 2009;30(1):71-76.
- Merck C, Angervall L, Kindblom LG, Odén A. Myxofibrosarcoma. A malignant soft tissue tumor of fibroblastic-histiocytic origin. A clinicopathologic and prognostic study of 110 cases using multivariate analysis. Acta Pathol Microbiol Immunol Scand Suppl. 1983;282:1-40.
- Weisong Li, Dan Li, Xiansen Zhu, Shaohui Lu, Chunlei He, Qingchun Yang. Low-grade myxofibrosarcoma following a metal implantation in femur: a case report, Diagnostic Pathology. 2014;9:6:2-8.
- Haglund KE, Raut CP, Nascimento AF,et al. Reccurence patterns and survival for patients with intermediate and high grade myxofibrosarcoma. Int J Radiation Oncology Biol Phys. 2012;82(1):361-367.