Introduction
Odontoid process fractures account for 10%-15% of all cervical fractures [
1]. Fractures involving the base of odontoid process is the most common [
2] and is classified as type II using the Anderson D’Alonso classification system [
3]. Non-operative treatment of these fractures has high complication rates such as non-union, pseudoarthrosis [
4-
6] along with pin tract infection, loosening of pins and other clinical complications associated to halo devices [
7-
8].
Posterior C1-C2 fusion will lead to loss of rotatory movement of cervical spine. The anterior odontoid screw fixation provides good anatomical and functional results with 90% expected union rates [
9-
11]. The main advantage with this method is preservation of rotatory movements of cervical spine. The surgical approach for anterior screw fixation involves dissection of prevertebral space and blind passage of screw, during which there is high chance of iatrogenic injury to the vital structures like carotid artery, trachea and esophagus. During entire surgical procedure simultaneous AP and lateral imaging is required. Hence the operating surgeon requires high expertise and skill to prevent damage to the vital structures along with a good theater set up.
Here we are highlighting the technical details of management of Type II odontoid fracture for which anterior screw fixation was done.
Case Report
A 19-year-old boy presented with complaints of severe neck pain and difficulty in neck movements following a road traffic accident. Cervical spine was initially stabilized with a Philadelphia collar. His neurological examination was unremarkable (ASIA grade E). Cervical radiography done, which showed Type II odontoid fracture with displacement [Fig.1] according to the Anderson and D’Alonso classification.
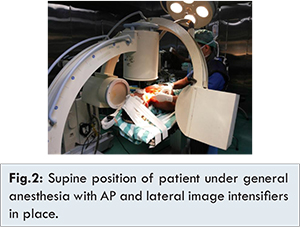
The imaging findings were discussed with the patient along with the pro’s and con’s of anterior and posterior surgical approaches. Anterior odontoid screw fixation was opted. General anesthesia with nasotracheal tube was given. Patient was in supine position and head stabilized with adhesive strap, on a radiolucent operating table with the mouth held open by placing cotton sponges in the mouth to get an open mouth view. Simultaneous AP and lateral fluoroscopy imaging was available throughout the surgery [Fig.2].
Anatomic reduction of the fragment was achieved by gentle flexion and extension maneuvers of the head along with transoral pressure by using solid instrument and reduction confirmed under fluoroscopy in both views. The operative field was prepared in a sterile manner, with sterile draping of both image intensifiers. 4 cm right anteromedial transverse skin incision made at the level of the C5-6 disc space. Platysma muscle was split longitudinally in line with its fibers. Blunt dissection of the pretracheal fascia was done and an interval was developed between the carotid sheath laterally and the strap muscles overlying the trachea, esophagus medially. Carotid sheath was retracted laterally and trachea, oesophagus medially done gently. Prevertebral space developed anteriorly along the front of the cervical spine until the anteroinferior margin of the C2 body was reached. Long drill sleeve inserted [Fig.3] at C2-C3 intervertebral disc space.

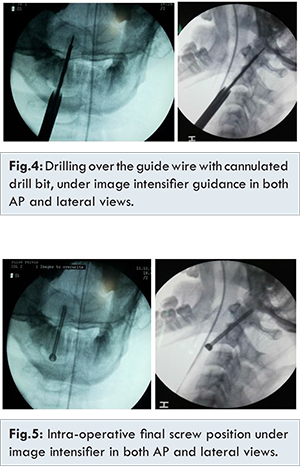
The desired entry point through the C2 endplate at the anteroinferior margin was confirmed under fluoroscopy in lateral view and centre of odontoid in AP view. Using a long drill sleeve, guide wire inserted under guidance of image intensifier. As we were planning for a single screw, we placed the guide wire in the middle of the odontoid in both anteroposterior, lateral view. Screw length was measured. Drilling was done up to the tip of odontoid with 4 mm cannulated drill bit [Fig.4]. Each forward movement of drill bit was checked regularly in C arm to know whether the guide wire is advancing to the brainstem. 4.5x50 mm fully threaded screw inserted over guide wire until the opposing apical cortical bone, under image intensifier [Fig.5]. The screw heads encroached on the anterior margin of the C2-3 intervertebral disc, into the disc space just inferior to the endplate.
Post-operative period was uneventful and his neurology was unremarkable. He was given two months of cervical immobilization followed by gradual mobilization and physiotherapy. Patient at one year follow up showed excellent results with painless cervical rotations and follow up radiographs [Fig.6] showed union of fracture.
Discussion
According to Anderson and D’Alonso [
3] classification type II odontoid fracture involves the base of odontoid process which is the most common and unstable type [
2,
3]. Grauer et al. [
12] further classified type II fractures into three subtypes mainly based on fracture line obliquity, displacement and comminution. Type IIA was defined as a minimally or non-displaced fracture with no comminution which could be treated with external immobilization. Type IIB was a displaced fracture extending from anterior-superior to posterior-inferior, or a transverse fracture which can be treated with anterior screw fixation after adequate fracture reduction. Type IIC was a fracture extending from anterior-inferior to posterior superior or a fracture with significant comminution which can be treated with posterior C1-C2 fusion.
Type I and Type III fractures are usually stable and may be treated conservatively with external immobilization in form of cervical collar or Halovest. Type II fractures are unstable and non-operative treatment has high complication rates such as nonunion and pseudoarthrosis [
4-
6]. Posterior C1-C2 fusion will lead to loss of rotatory movement of cervical spine. Anterior odontoid screw fixation provides good anatomical and functional results with 90% expected union rates [
9-
11]. The main advantage with this method is the preservation of rotatory movements of the cervical spine. By using Robinson smith approach [
13], a transverse incision placed at the level of C5-C6 disc space to prepare a working corridor to C2 level.
Fracture reduction is mandatory before anterior screw fixation. This approach is contraindicated in comminuted axis body fractures, oblique fractures, reverse type of odontoid fracture pattern, pathological fractures, non-union, short neck, kyphotic neck, obese people, children younger than 7 years and rupture of transverse atlantal ligament [
14]. Osteopenia in elderly patients is a relative contraindication [
14]. Rare complications with this approach are screw malposition, screw fracture, screw pull out [
15].
Few authors proposed two screws for these fractures [
4,9], But Sasso et al. in their biomechanical studies have found no significant differences between one and two screw placements [
16].
Conclusion
Anterior screw fixation for Type II odontoid fracture is an excellent treatment option, provided that surgery is well planned with meticulously executed fixation by an experienced surgeon helps to provide osteosynthesis and near normal anatomy. Hence provides better functional results.
References
- Maak TG, Grauer JN. The contemporary treatment of odontoid injuries. Spine(Phila Pa 1976). 2006;31(11 Suppl):S53-60
- Hadley MN, Dickman CA, Browner CM, Sonntag VK. Acute axis fractures: a review of 229 cases. J Neurosurg. 1989;71(5 Pt 1):642-647.
- Anderson LD, D’Alonzo RT. Fractures of the odontoid process of the axis. J Bone Joint Surg Am. 1974;56(8):1663-1674.
- Seljeskog EL. Non-operative management of acute upper cervical injuries. Acta Neurochir (Wien). 1978;41(1-3):87-100.
- Schweigel JF. Management of the fractured odontoid with halo-thoracic bracing. Spine (Phila Pa 1976). 1987;12(9):838-839.
- Fujii E, Kobayashi K, Hirabayashi K. Treatment in fractures of the odontoid process. Spine (Phila Pa 1976). 1988;13(6):604-609.
- Majercik S, Tashjian RZ, Biffl WL, Harrington DT, Cioffi WG. Halo vest immobilization in the elderly: a death sentence? J Trauma. 2005;59(2):356-358.
- Chapman J, Smith JS, Kopjar B, Vaccaro AR, Arnold P, Shaffrey CI, et al. The AO Spine North America Geriatric Odontoid Fracture Mortality Study: a retrospective review of mortality outcomes for operative versus nonoperative treatment of 322 patients with long-term follow-up. Spine (Phila Pa 1976). 2013;38(13):1098-1104.
- Apfelbaum RI, Lonser RR, Veres R, Casey A. Direct anterior screw fixation for recent and remote odontoid fractures. J Neurosurg. 2000;93(2 Suppl):227-236.
- Hénaux PL, Cueff F, Diabira S, Riffaud L, Hamlat A, Brassier G, Morandi X. Anterior screw fixation of type IIB odontoid fractures in octogenarians. Eur Spine J. 2012;21(2):335-339.
- Julien TD, Frankel B, Traynelis VC, Ryken TC. Evidence-based analysis of odontoid fracture management. Neurosurg Focus. 2000;8(6):e1.
- Grauer JN, Shafi B, Hilibrand AS, Harrop JS, Kwon BK, Beiner JM, et al. Proposal of a modified, treatment-oriented classification of odontoid fractures. Spine J. 2005;5:123-129.
- Etter C, Coscia M, Jaberg H, Aebi M. Direct anterior fixation of dens fractures with a cannulated screw system. Spine (Phila Pa 1976). 1991;16(3 Suppl):S25-32.
- Arnold PM, Haynes NG, Kelley BC. Youmans neurological surgery. 6th ed. Philadelphia: Elsevier; 2011. pp. 3194.
- Lee EJ, Jang JW, Choi SH, Rhim SC. Delayed pharyngeal extrusion of an anterior odontoid screw. Korean J Spine. 2012;9(3):289-292.
- Sasso R, Doherty BJ, Crawford MJ, Heggeness MH. Biomechanics of odontoid fracture fixation. Comparison of the one- and two-screw technique. Spine (Phila Pa 1976). 1993;18(14):1950-1953.