|
|
|
|
|
Importance of Identifying Physiological Preputial Adhesion and Pathological Phimosis as Different Clinical Entities in Children
|
|
|
when to use naloxone vs naltrexone naloxone vs naltrexone
Departments of Surgery1 and Paediatrics2, Nehru Shatabdi Central Hospital, Talcher, Angul, Odisha 759103, India and Department of Paediatrics3, Central Hospital, Barajamda, West Singhbum, Jharkhand, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Sandip Kumar Rahul
Email: sandeep.rahul65@gmail.com
|
|
|
|
|
|
|
|
|
Received:
20-APR-2016 |
Accepted:
27-JUN-2016 |
Published Online:
30-AUG-2016 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Objective: To assess the importance of identifying physiological preputial adhesion and pathological phimosis as different clinical entities in children. Methods: A prospective study was done on 40 patients of presumed phimosis, referred to the paediatric surgery department, for circumcision. Patients were examined for their symptoms and classified as either having symptomatic physiological preputial adhesions or pathological phimosis. Patients in the former group underwent adhesiolysis and those in the later group underwent circumcision. They were followed up and results obtained were analysed. Results: Out of the 40 patients referred with a presumed diagnosis of phimosis, only 5 (12.5%) patients had pathological phimosis and among these 3 were found to have balanitis xerotica obliterans. Pathological phimosis patients presented late at a mean age of 60 months. They underwent circumcision. 35 (87.5%) patients were found to have symptomatic physiological preputial adhesions and presented earlier at a mean age of 28 months. 33 (94.3%) of these could be managed by simple adhesiolysis as outdoor patients while 2 patients were non-responders and needed circumcision. Among responders to adhesiolysis, majority of the patients (29 out of 33) needed a single attempt while 4 patients needed multiple attempts at adhesiolysis. Conclusion: Most of the patients referred for circumcision for phimosis actually had symptomatic preputial adhesions which could be managed by simple adhesiolysis. Only few patients had pathological phimosis needing circumcision. Balanitis xerotica obliterans was found to be an important cause of pathological phimosis. Proper diagnosis could prevent unnecessary surgical intervention under anaesthesia and keep the prepuce intact preserving its vital functions.
|
|
|
|
|
|
Keywords :
|
Balanitis Xerotica Obliterans, Child, Circumcision, Penile Diseases, Phimosis.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffa4fa0f000000f204000001000900 6go6ckt5b5idvals|654 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Circumcision is a common surgical procedure in paediatric patients. If religious circumcision is left out, then only a few medical indications remain for circumcision. Although there are known benefits of circumcision, there are known functions of an intact prepuce as well [1-4]. It is, therefore, very important to identify a patient who actually has a need for circumcision. Physiological preputial adhesions (PPA) and pathological phimosis (PP) are both common in children. While the former is physiological and needs treatment only when causing any secondary problem, the later often needs circumcision. Adhesiolysis suffices for symptomatic PPA and can usually be done under topical anaesthetics like lignocaine. On the other hand, PP needs procedures like circumcision, dorsal slit and preputioplasty for which general anaesthesia is needed in paediatric patients. Proper diagnosis of the condition is important to avoid the unnecessary surgical and anaesthetic procedure.
Through this study, we aimed to identify the over diagnosis of phimosis by primary physicians and the need to categorize these patients into those having PPA and PP. This would bring down the number of unnecessary circumcision.
Material and Methods
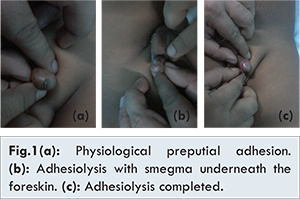
This was a prospective study conducted on 40 patients referred for pediatric surgery consultation in a tertiary care hospital for phimosis during 6 month period. Patients with asymptomatic PPA and those referred for ritual circumcision were not included in the study. Data, regarding age and chief complaints, were obtained. These patients were found to present with three main symptoms - ballooning of foreskin, difficulty in micturition and features of urinary tract infection. Patients were examined for their complaints and were classified as either having PPA or PP. Routine urine and culture examinations were done in patients having features of urinary tract infection. Patients, in whom, the foreskin was thin and supple and could be gently separated from the glans as an outdoor procedure under local lignocaine were considered to have PPA and the procedure was called ‘preputial adhesiolysis’ [Fig.1]. Patients having thick, fibrotic and tight foreskins which could not be gently separated and retracted from the glans were considered to have PP and circumcision was done in these patients under anaesthesia. Patients with PPA who had adhesiolysis were followed and their parents were encouraged to retract and clean the prepuce once daily. Cases, in which adhesions recurred and retraction again became difficult, were circumcised. The results obtained were then analyzed.
A total of 40 patients with age ranging from 6 months to 80 months and a mean age of 32 months came for consultation. 35 (87.5%) of these patients were found to have PPA, while only 5 (12.5%) patients actually had PP. Figure 2 shows the summary of results. PPA patients were found to present at a mean age of 28 months. Compared to this, patients with PP presented late at a mean age of 60 months. 25 patients presented with ballooning of prepuce, 14 patients had difficulty in micturition and 5 presented with urinary tract infection.
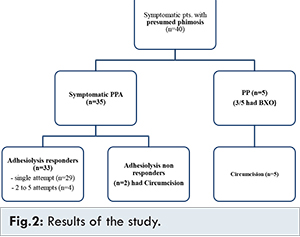
Preputial adhesiolysis was initially tried in all patients with PPA. Among these, in 29 patients only a single attempt at adhesiolysis was sufficient. 4 other patients needed 2 to 5 attempts at adhesiolysis. 2 patients did not respond even to multiple attempts of adhesiolysis and in them, finally circumcision had to done. 3 of the 5 PP patients were found to have thick unyielding and scarred foreskin with grey white discoloration of glans and foreskin [Fig.3]. One of these patients was found to have meatal stenosis. These 3 patients were found to have balanitis xerotica obliterans (BXO). All the 5 patients with PP underwent circumcision. In one patient of BXO having meatal stenosis, meatotomy was additionally required.
Discussion
Prepuce develops as a bilayered investment between 8 to 16 weeks of gestation. It arises as a result of distal folding of the integument covering the penis on itself [5]. Initial separation of the prepuce from the glans starts as early as 24 weeks of gestation but the inner preputial layer and glans appear adherent at birth [5]. By the process of keratinisation and desquamation these two stratified squamous layers gradually separate and usually the time period for complete separation is variable. At birth, only four percent have completed this separation; by 6 months, 20%; by 3 years, 90 percent and by 17 years, 99 percent [6,7]. So, PPA is expected to resolve on its own keeping this natural process of separation in mind. However, urinary symptoms of thin stream, difficulty in voiding and urinary tract infections can result if preputial adhesions impede the urinary flow. Also, infection of smegma underneath the foreskin and balano-posthitis can occasionally occur. It is this small group of patients with PPA that would benefit from gentle adhesiolysis and proper after care by the parents. Circumcision under general anaesthesia is unnecessary in such patients. It exposes the child to the risks of anaesthesia and adverse effects of circumcision.
Penile foreskin serves protective, immunologic and erogenous function. Numerous glands and Langerhans cells present in prepuce are instrumental in protective and immunologic functions [2,3]. Glans and the external urethral meatus nested in it are naturally shielded from external trauma by the prepuce. It has sensitive touch receptors, rich vascular and nerve supply [4]. Sacrificing it by misdiagnosing PPA as PP would mean a loss of all these vital functions. Not all children with PPA need adhesiolysis. It should only be done in patients who have secondary symptoms due to PPA like difficulty in micturition and recurrent urinary tract infection. Ballooning of prepuce is now considered to be indicative of separation of prepuce and glance. A forcible attempt to retract the prepuce in a case of PPA where it is not needed does more harm than good. It may lead to micro-tears, infection and bleeding with secondary scarring resulting in PP.
If the foreskin is thick and unyielding, PP is considered. It is often the result of poor hygiene, recurrent balanitis, posthitis or balano-posthitis. BXO is a variant of Lichen sclerosus et atrophicus involving the male external genitalia to different extent. Phimosis secondary to BXO is severe and there may also be involvement of the glans, meatus and urethra [8]. In cases of PP, non-surgical management with topical steroid medications like betamethasone have been tried with variable results [9]. Effects have been attributed to the anti-inflammatory and immunosuppressive properties of steroids. Circumcision under general anaesthesia is considered in steroid unresponsive cases or sometimes even as the primary treatment option. BXO patients benefit from circumcision but may need additional procedures like meatal dilatation, meatotomy, meatoplasty, urethrotomy or urethroplasty with buccal graft depending on the extent of involvement of the meatus, glans and urethra [8]. Foreskin removed at circumcision should be sent for histopathological examination. Evidence of BXO was found in the foreskin of three of our PP patients.
Proper examination and identification of the patient’s condition is therefore very important to avoid unnecessary surgery and risky anaesthesia. It has been a general trend worldwide to misdiagnose PPA as PP and subject these patients to circumcision when they could have easily been managed by adhesiolysis as an outdoor procedure [10-12] . That the number of medically indicated circumcision has been seven times the observed incidence of phimosis in children less than 15 years of age reflects the magnitude of the problem [11]. This also has a huge economic impact [13]. In a study from the Indian subcontinent, Kumar et al. found a trend towards referral for circumcision due to incorrect diagnosis of preputial adhesions as phimosis [14]. Our results were consistent with these investigators.
We concluded that most of the patients were erroneously diagnosed to have phimosis and were referred for circumcision by primary physicians. This shows a lack of awareness among them about PPA as an entity separate from PP and that it can be managed with a simpler procedure compared to circumcision. Patients with PPA were younger compared to PP patients. Only symptomatic cases of PPA needed treatment. Most of them could be managed by a single attempt at adhesiolysis without any significant complication. BXO was found to be an important cause of PP in children.
References
- Van Howe RS. Is neonatal circumcision clinically beneficial? Argument against. Nat Clin Pract Urol. 2009; 6:74-75.
- Fleiss PM, Hodges FM, Van Howe RS. Immunological functions of the human prepuce. Sex Transm Infect. 1998; 74:364-367.
- Cold CJ, Taylor JR. The prepuce. BJU Int. 1999; 83:34-44.
- Sorrells ML, Snyder JL, Reiss MD, Eden C, Milos MF, Wilcox N, Van Howe RS. Fine-touch pressure thresholds in the adult penis. BJU Int. 2007; 99:864-869.
- Yiee JH, Baskin LS. Penile embryology and anatomy. Scientific World Journal. 2010; 10:1174-1179.
- Oster J. Further fate of the foreskin. Incidence of preputial adhesions, phimosis and smegma among Danish schoolboys. Arch Dis Child. 1968;43:200-203.
- Malone P, Steinbrecher H. Medical aspects of male circumcision. BMJ. 2007; 335:1206-1290.
- Hartley A, Ramanathan C, Siddiqui H. The surgical treatment of Balanitis Xerotica Obliterans. Indian J Plast Surg. 2011;44:91-97.
- Marques TC, Sampaio FJ, Favorito LA. Treatment of phimosis with topical steroids and foreskin anatomy. Int Braz J Urol. 2005;31:370-374.
- Rickwood AM, Kenny SE, Donnell SC. Towards evidence based circumcision of English boys: survey of trends in practice. BMJ. 2000;321:792-793.
- Spilsbury K, Semmens JB, Wisniewski ZS, Holman CD. Circumcision for phimosis and other medical indications in Western Australian boys. Med J Aust. 2003;178:155-158.
- Huntley JS, Bourne MC, Munro FD, Wilson-Storey D. Troubles with the foreskin: one hundred consecutive referrals to paediatric surgeons. J R Soc Med. 2003;96:449-451.
- Steadman B, Ellsworth P. To circ or not to circ: indications, risks, and alternatives to circumcision in the pediatric population with phimosis. Urol Nurs. 2006;26:181-194.
- Kumar P, Deb M, Das K. Preputial adhesions a misunderstood entity. Indian J Pediatr. 2009; 76:829-832.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Rahul SK, Behera S, Mohapatra S, Suman PImportance of Identifying Physiological Preputial Adhesion and Pathological Phimosis as Different Clinical Entities in Children.JCR 2016;6:401-405 |
|
Rahul SK, Behera S, Mohapatra S, Suman PImportance of Identifying Physiological Preputial Adhesion and Pathological Phimosis as Different Clinical Entities in Children.JCR [serial online] 2016[cited 2026 Jun 13];6:401-405. Available from: https://www.casereports.in/articles/6/3/Importance-of-Identifying-Physiological-Preputial-Adhesion-and-Pathological-Phimosis-as-Different-Clinical-Entities-in-Children.html |

|
|
|
|
|