Introduction
Leiomyoma is the most common of all uterine and pelvic tumors. The incidence of leiomyoma is 20% in the reproductive age group, and only 1-2% are found in the cervix [
1]. Cervical fibroid develops usually in the supravaginal part of cervix [
2]. The symptoms most commonly presented are retention of urine, menstrual abnormalities, constipation, and sometimes can present only as an abdominal mass without any other symptoms and may mimic an ovarian tumor [
3,
4]. Large cervical fibroids are rare and can present with surgical difficulties at the time of either myomectomy or hysterectomy and have an increased risk of urinary tract injuries and intraoperative bleeding. We hereby present one such case of large cervical fibroid who underwent a hysterectomy successfully.
Case Report
A 30-year woman, married since 15 years, para 4, living 4, abortion 1 with tubal ligation done 2 years back, presented with a history of insidious onset abdominal pain for last 1 year and menorrhagia. She had no bowel or urinary complaints. General and systemic examination revealed no abnormality. Per-abdomen examination revealed a mass of about 24 weeks size gravid uterus, which was non-tender, solid in consistency with restricted mobility. Lower margin of mass was not palpable. There were no palpable ascites. On per speculum examination, part of cervical fibroid was seen posteriorly through the cervical os. On bimanual examination, there was a large solid mass filling the pelvic cavity and extending into the abdomen up to the umbilicus. Uterus could not be felt separately from the mass. On investigation hemoglobin was 11.4 g/dL, liver and renal function tests were normal. Ultrasound report showed a bulky uterus measuring 13x8.5x7.8 cm and a solid lesion of 14.5x10x8 cm in the cervix arising from posterior wall suggestive of a cervical fibroid.
Initially she was posted for hysteroscopy, endometrial sampling and cervical biopsy to investigate menorrhagia. However, dilatation and curettage or hysteroscopy was not possible due to the fibroid and hence only cervical biopsy was taken which showed chronic cervicitis on histopathology. Subsequently, she was posted for assessment under anaesthesia regarding route of hysterectomy. The plan was to assess if we could open pouch of Douglas (POD) and get access to the lower segment fibroid to enucleate it. However, we could not reach the POD and hence decision to do a total adomninal hysterectomy was taken.
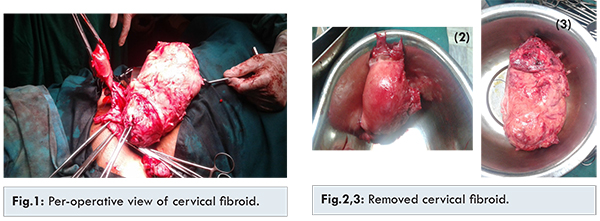
Abdominal hysterectomy under spinal anesthesia revealed large cervical fibroid 15 cm x 10 cm x 5 cm in size [Fig.1]. Uterus was normal in size (4x2x2 cm) with normal ovaries and fallopian tubes. Uterus was sitting on the top of the fibroid and was pushed upward. Cervix was elongated. A transverse incision was made anteriorly in the capsule of fibroid and the bladder was dissected down. A 2 kg cervical fibroid was removed by enucleation of the capsule by blunt dissection with finger and hemostasis of fibroid bed [Fig.2,3]. Care was taken to remain within the capsule so as to avoid ureteric injury. Left ureter was found to be stretched around the fibroid midway along its length. Careful dissection of ureter and bladder was done before ligating any of the pedicles. Total abdominal hysterectomy with right sided salpingo-oophorectomy was done. Patient received two units of blood intra-operatively. Her post-operative period was uneventful. Histopathological examination confirmed a cervical fibroid with hyaline change.
There are very few cases of large cervical fibroids posted in the literature. Sharma et al. from Sri Lanka reported a case of cervical fibroid measuring 30x26x22 cm that clinically resembled an ovarian tumor. Patient presented with abdominal distention and loss of weight. During surgery, left ureter was injured and ureteric anastomosis was done [
6]. Basnet et al. in Nepal also reported a case of huge cervical fibroid of 30x14x10 cm with an unusual presentation. In their case patient had gradual abdominal distention, scanty and irregular menstruation and no bowel and bladder complaints. During surgery bladder injury occurred that was repaired and to achieve hemostasis bilateral internal iliac arteries were ligated [
7].
In our case, the cervical fibroid was smaller than the above two. Presentation was not unusual (pain, distention and menorrhagia) [
3,
4]. Ideally, such cervical fibroids should be investigated with a CT scan to get a better idea of the location, extent and proximity to ureters. However, based on the presentation and clinical findings we felt it was more of a lower uterine fibroid rather than cervical fibroid and hence the attempt to assess the route of hysterectomy under anaesthesia was undertaken which in retrospect was not the right decision. Access to pouch of Douglas is possible in lower uterine fibroids where the peritoneal reflection is below the lower border of the fibroid as compared to cervical fibroid where the peritoneal reflection is above the upper border of the fibroid and hence inaccessible.
Dissecting and enucleating a large fibroid (whether cervical or uterine) by limiting the dissection to within the capsule of the fibroid is a key surgical technique to prevent ureteric injury in addition to careful dissection of ureters and bladder and clamping any pedicle with keeping ureters under direct vision.
Conclusion
Large cervical fibroids are a very rare scenario and require an expert hand to operate them to avoid blood loss, prevent inadvertent injury to ureters or the bladder.
References
- Bhatla N. Tumours of the corpus uteri. In: Jeffcoates Principles of Gynaecology. 5th ed. London: Arnold Publisher; 2001. pp. 470.
- Tiltman AJ. Leiomyoma of uterine cervix: A study of frequency. Int J Gynaecol. 1998;17:231-234
- Suneja A, Taneja A, Guleria K, Yadav P, Agarwal N. Incarcerated procidentia due to cervical fibroid: An unusual presentation. Aust N Z J Obstet Gynaecol. 2003;43:252-253.
- Dutta DC. Benign lesions of the uterus. In: Textbook of Gynaecology including Contraception. 3rd ed. India: New Central Book Agency (p) Ltd; 2004. pp. 264.
- Shirsagar SN, Laddad MM. Unusual presentation of cervical fibroid: Two case reports. Int J Gynaecol Plastic Surg. 2011;3:38-39.
- Sharma S, Pathak N, Goraya SP, Singh A, Mohan P. Large Cervical fibroid mimicking an ovarian tumor. Sri Lanka J Obstet Gynaecol. 2001;33:26-27.
- Basnet N, Bannerjee B, Badami U, Tiwari A, Raina A, Pokhare H, et al. An unusual presentation of huge cervical fibroid. Kathmandu Univ Med J (KUMJ). 2005;3:173-174.