Introduction
The term fetus papyraceus is used when intrauterine demise of a twin early in pregnancy occurs with retention for a minimum of 10 weeks resulting in mechanical compression resembling parchment paper [
1]. Fetus papyraceus is a rare complication with a reported incidence of one in 12,000 pregnancies [
2] and between 1:180 and 1:200 twin pregnancies [
3]. If the fetus is absorbed completely, no complications other than first trimester bleeding occur [
4-
6]. However if the event occurs in the second or third trimester, serious complications may include premature labour, infection due to the death of the fetus and hemorrhage [
4-
6]. Even at the end of the pregnancy, a low-lying fetus papyraceus may block the cervix and require a cesarean section to deliver the living twin. We hereby report conservative management of fetus papyraceus.
Case Report
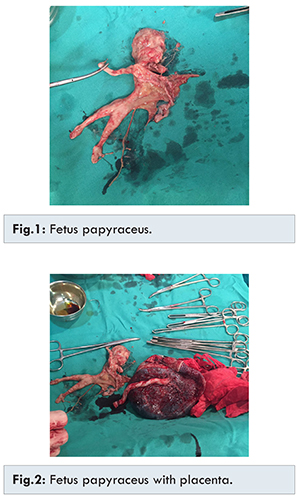
A G2A1, 24-year-old patient presented to our outpatient clinic after conception. She married at the age of twenty and had a past history of missed abortion at six weeks gestation. She gave history of evacuation and failed to conceive for about two years. Subsequently, hydrotubation was done twice and she was prescribed clomiphene citrate. Routine antenatal examinations were done regularly. The patient underwent regular antenatal care and ultrasound examination at the tenth month of gestation showed a single live intrauterine fetus with an estimated gestation of 9 weeks and no anomalies. Routine examinations and the coagulation profile were within normal limits. Another ultrasound done at eighteen weeks revealed twin live intrauerine fetuses of gestation age 17 weeks and 15 weeks respectively. Regular antenatal monitoring was continued. Coagulation profile repeated was normal. Sonography done at 30 weeks showed one live fetus in cephalic presentation with biparietal diameter corresponding to 28 weeks, femur length corresponding to 29 weeks and head circumference: 27 weeks with upper segment early Grade 3 placenta and liquor in lower limit of normal. The other twin was fetus papyraceus corresponding to 18 weeks gestation. Routine examinations and all routine biochemical investigations including coagulation profile were within normal limits. The patient was counseled on the principles of ethical decision making and she decided for conservative management. Hemogram, prothrombin time, activated plasma thromboplatin time, fibrin degradation products and serum fibrinogen levels were all within normal limits. She was given two doses of betamathasone at twenty four hours interval at 32 weeks. Lower segment cesarean section (LSCS) was done at 36 weeks and healthy normal male baby was delivered. The baby cried immediately after birth and was transferred to Neonatal Intensive Care Unit for further management. It was a diamniotic dichorionic twin gestation with one sac having fetus papyraceus [Fig.1,2].
High resorption rate in multiple pregnancies, suggest intense competition for space, nutrition, or other factors during early gestation, with frequent loss or desorption of the other twin [
5]. The fetus papyraceus, vanishing or mummified twin can be diagnosed early during antenatal care visits by imaging studies such as ultrasonography. However, ultrasound has technical difficulties and is affected by the anatomical position of the dead fetus. In the first trimester, this may be present as vaginal bleeding. But in the second and third trimesters, it is usually associated with several complications such as preterm labor, hemorrhage, sepsis as a result of dead fetus, consumptive hemorrhage and labor dystocia. These complications become severe when it is a monochorionic placenta rather than dichorionic placenta [
3,
6]. In our case it was dichorionic placenta and there was no such complication.
In monochorionic twinning, the surviving twin is at risk of complications like cerebral palsy, aplasia cutis, congenital malformations such as microcephaly or hydrocephalus. This may occur due to transfusion of thromboplastic proteins from the vanishing twin to the surviving twin, leading to disseminated intravascular coagulation (DIC) and subsequent intrauterine central nervous system damage [
7-
9]. Another proposed mechanism of central nervous system damage involves large amount of blood loss from the surviving twin to the low resistance system of the vanishing twin through placental anastomosis. This transfusion could cause wide fluctuation in intravascular pressure, leading to intraventricular hemorrhage which may result in cerebral palsy [
10].
Our case was a treated case of secondary infertility, already having a fetal loss, we took no risk and did elective LSCS at maturity before any complication could have occurred. Since it is hypothesized that in some instances vanishing twins leave no detectable trace at birth or before, it is impossible to say for certain how frequent the phenomenon is. It was hypothesized for a long time that the left handed individuals may be survivors of “mirror image” identical twinning [
11].
Vanishing twins are frequently encountered in the pregnancies created as a result of in-vitro fertilization. Ultrasound scans taken early in these pregnancies show multiple conception whereas a few weeks later there is only one amniotic sac and the other has vanished [
12].
Conclusion
The primary concern for the fetus papyraceus is its effect on the surviving fetus and on the mother. To avoid possible complications, intrauterine diagnosis of fetus papyraceus by serial ultrasound examinations to search for the fetus papyraceus is mandatory.
References
- Dickey RP, Tailor S, Lu PY, Sartor BM, Rye PH, Storment JM, Rye PH, et al. Spontaneous reduction of multiple pregnancy: incidence and effect on outcome. Am J Obstet Gynaecol. 2002;186(1):77-83.
- Rathi BA, Rathi S. Fetus papyraceus- Acase report. J Obs Gynaecol India. 2003;53:188
- Woo HH, Sin S, Tang LC. Single fetal death in twin pregnancies: review of maternal neonatal outcome and management. Hong Kong Med J. 2000;6(3):293-300.
- Landy HJ, Weiner S, Corson SL, Batzer FR. The “vanishing twin”: ultrasonographic of fetal disappearance in the first trimester. Am J Obstet Gynecol. 1986;155(1):14-19.
- Pelega D, Ferber A, Orvieto R, Bar-Hava, I. Single intrauterine fetal death (fetus papyraceus) due to uterine trauma in a twin pregnancy. European Journal of Obstetrics & Gynecology and Reproductive Biology. 1988;80(2):175-176.
- Dahiya P, Ranjita B. Conservative management of fetus payraceus: a report of two cases. Oman Med J. 2014;29(2):132-134.
- Classen D. Aplasia cutis congenital associated with fetus payraceus. Cutis. 1999;64(2):104-106.
- Pharaoh P. Prevalence and pathogenesis of congenital anomalies in cerebral palsy. Arch Dis Child Fetal Neonatal Ed. 2007;92(6):F489-93.
- Benirschke K. Intrauterine death of a twin: mecahanism, implication for surviving twin, and placental pathology. Semin Diagn Pathol. 1993;10(3):222-231.
- Anand D, Platt M, Pharoah P. vanishing twin: a possible couse of cerebral impairment. Twin Res Hum Genet. 2007;10(1):202-209.
- Newman HH. Studies of Human Twins II. Asymmetry Reversal, of Mirror Imaging in Identical Twins. Biological Bulletin. 1928;55(4):298-315.
- Jauniaux, E, Elkazen N, Leroy F, Wilkin, P. Clinical and morphologic aspects of the vanishing twin phenomenon. Obstetrics & Gynecology 1988;72(4):577-581.