Introduction
Ureteroscopic stone removal is a widely accepted method as first line treatment for many patients with ureteric calculi [
1]. Various types of stone grasper forceps or baskets are used to extract stones, stone fragments or to bring down the migrating stone in dilated ureter [
2]. Despite the new smaller semi-rigid ureteroscopes and availability of various methods of retrieval and fragmentation of stones, surgical misadventures still occur [
3]. In literature, complications related to stone retrieval forceps have been described pertaining only to baskets. We describe two cases of malfunctioning of rigid triprong grasper forceps (entrapment in one case and detachment of open triprong forceps with its stem from body in another case) managed successfully with ureteroscopy.
Case Reports
We report two cases of ureteric injuries caused by triprong stone removal forceps. One injury was due to spontaneous dismantling of triprong assembly while catching the stone fragment, while the second one was due to entrapment and disassembly of triprong forceps containing the stone fragment within. The triprong forceps used, were of two different types. The parts of triprong forceps are outer sheath, inner rod with three prongs at its end and a handle with spring action [Fig.1]. The inner rod can be of two types - one consisting of the three prongs integrated with the system [Fig.1] and another type where the prongs are separately attached to the stem of inner rod. We used ureteroscopes of sizes 8F and 8/9.5 Fr.
Case 1
A 28 year old male known case of left lower ureteric stone, 8 mm in size, was posted for left ureteroscopy. Ureteroscopy was done with semi-rigid ureteroscope, 8/9.5 Fr. After placing a safety 0.035 Fr guide wire, the stone was fragmented into two. On attempting removal of these fragments with the triprong forceps, the stem accidentally detached from the body within the dilated ureter.
The URS and the dismantled body of triprong forceps were removed and a new smaller sized 8F semi-rigid ureteroscope was reintroduced. A new rigid biprong stone removal forceps was inserted, and the three dismantled prongs were brought into the closed position and this assembly was removed by holding the stem of triprong, under vision without any ureteric injury. A retrograde pyelogram showed no extravasation of contrast. A 5 Fr, 26 cm Double J (DJ) stent was placed, which was removed after 6 weeks. Patient remained asymptomatic without having any stricture or obstruction at 6 months follow-up.
Case 2
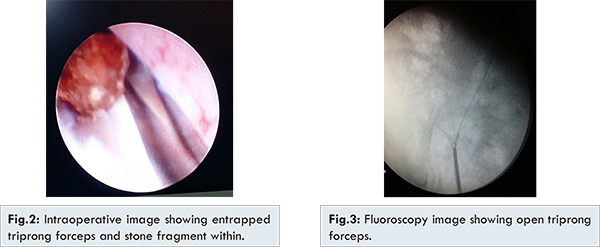
A 60 years old male, having a left 1.2 cm mid ureteric stone, was posted for ureteroscopy and insitu lithotripsy (URSL). Ureteroscopy was done with 8/9.5 Fr rigid ureteroscope after 0.035 safety guide wire. The stone was freely mobile in the dilated ureter and had retropulsive mobility. To avoid this retropulsion, 4 Fr rigid triprong forceps was used to bring it down. However, the triprong forceps got entrapped in mid ureter, with stone within its clasp [Fig.2,3]. While trying to free the prongs of the forceps from the stone, the spring at the handle gave way and sheath got detached from the central rod. The central rigid rod with open prongs containing the stone got stuck in the mid-ureter. We removed the outer sheath and ureteroscope. Beside the central rod, a new smaller sized 8 Fr semi-rigid ureteroscope was reintroduced upto the stone and the stone was fragmented completely. Using rigid biprong stone removal forceps, all the three prongs were brought together in the ureteral lumen. Ureteroscope and triprong forceps were removed under vision. Ureteroscope was reintroduced and ureter was inspected for any injury. There was ureterotomy of size approximately 1 cm by one of the prongs on posterior wall, no other injury. Retrograde pyelogram (RGP) showed no extravasation of contrast. 5 Fr, 26-cm DJ stent was inserted which was later removed after 6 weeks. While removing the stent, RGP was done which showed normal caliber of ureter and non-obstructed drainage. Patient remained asymptomatic without having stricture or obstruction at 6 month follow-up.
Ureteroscopy has evolved dramatically in technique and instrumentations, and has gained a prominent role in management of urolithiasis [
3]. When feasible, baskets or rigid triprong forceps are used as rapid means of stone retrieval. Intra-operative complications include inability to gain access to the ureter or negotiate vesico-ureteric junction, inability to reach the stones, migration of stones, perforation of ureter, avulsion of ureter, entrapment of stone retrieval forceps [
2]. Blind basketing of ureteric calculi using fluoroscopy imaging, the procedure previously used before the introduction and widespread use of ureteroscopes, used to get complicated by entrapment in around 1% of cases. In a study by Geavlete et al. in 2735 ureteroscopic procedures, incidence of trap stone extractors was 0.7% and overall rate of intra-operative complications was 3.8% [
3]. Various instruments for stone retrieval have been in use for instance baskets, triprong multi-wire grasper, and biprong forceps. Unfortunately published data on the retrieval capability and safety features of different instruments are rare [
2]. Triprong grasper, instead of basket, may prevent the major complications. The use of grasper prevents entrapment, breakage, and avulsion as with excessive force the stone pops out of the grasper [
2]. In both of our cases, rigid triprong forceps were used for stone retrieval during ureteroscopy,but in both cases triprong grasper forceps malfunctioned.
Various methods have been described for the removal of entrapped stone baskets in literature like ureterolithotomy, ureteral meatotomy, Shock Wave Lithotripsy (SWL) for stone [
5] and ureteroscopy [
2]. Entrapment is due to overfilling of forceps with single large or multiple small stones [
1]. So avoidance of catching the stone or stone fragment which is too large to remove in one piece is the best method of prevention, however even in best hands this complication may occur [
4]. In our case, we have described use of small sized 8 Fr ureteroscope and biprong forceps to bring down the open prongs of entrapped triprong close to each other in lumen after fragmentation of entrapped stone in it and removal under vision. By using ureteroscope, entrapped forceps and its contents can be visualized directly which facilitates its safe removal. Availability of small sized ureteroscope improves ability to manipulate instrument in difficult areas. Injury can be assessed after removal of forceps and stone by reinserting the ureteroscope. Entrapped forceps occasionally caught in ureteral mucosa can be visualized endoscopically which may help in safe removal of forceps and avoid further injury [
1]. Various minor and major complications can occur due to entrapment of triprong forceps, like minor mucosal injury to avulsion of ureter [
2]. Minor mucosal injuries due to forceps are self-limiting and minor perforations can be managed by ureteral stenting for 3-6 weeks and antibiotics as like in our case. Dense ureteral stricture may occur as late complication of ureteroscopy in 0.5-2.5% [
2]. However in our case, at the end of 6 months, while removal of stent, intravenous pyelography (IVP) and RGP were normal.
Principles for prevention of complications during stone retrieval by triprong forceps [
2] include: checking forceps prior to its use, use of guide wire, fragmenting of stone to very small sizes, avoiding forceful retrieval of large stones, fluoroscopic monitoring and sound endoscopic judgement.
Conclusion
Entrapment of triprong forceps while removing the stones during ureteroscopy is a rare but devastating complication. Urologist must be aware of such complication and various methods of its management. The best way to prevent this type of complication is careful attention to instrument selection and avoidance of overzealous and indiscriminate manipulations of instruments.
References
- O’Connor RC, Gerber GS. Management of entrapped ureteral stone baskets. Tech Urol. 2000;6(3):231-233.
- de la Rosette JJ, Skrekas T, Segura JW. Handling and prevention of complications in stone basketing. Eur Urol. 2006;50(5):991-998; discussion. 998-999.
- Geavlete P, Georgescu D, Nita G, Mirciulescu V, Cauni V. Complications of 2735 retrograde semirigidureteroscopy procedures: a single-center experience. J Endourol. 2006;20(3):179-185.
- Durano AC, Hanosh J. A new alternative treatment for entrapped stone basket in the distal ureter. J Urol. 1988;139:116-117.
- Low RK, George D. Removal of the entrapped basketed ureteral calculus: a novel technique. J Urol. 2000;163(6):1863.