Introduction
Hodgkin’s lymphoma is one of the two common types of cancers of the lymphatic system. The other type, which is far more common, is called as the non-Hodgkin’s lymphoma (NHL). CNS involvement by Hodgkin’s lymphoma is extremely rare, with estimated incidence of less than 0.5%. A recent German study on Hodgkin’s lymphoma comprising of more than 14,000 patients showed only 0.2% CNS involvement [
1]. It is generally a late manifestation and represents a serious and potentially fatal complication for the patient. Here, we present a rare case of a Hodgkin’s lymphoma patient with CNS (cerebellar) involvement.
Case Report
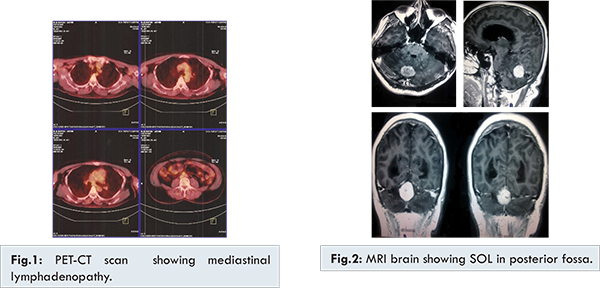
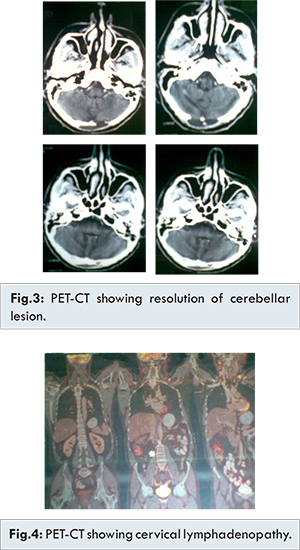
A 46-year old male presented with anorexia and cervical lymphadenopathy. There was no history of fever, cough, weight loss or significant past medical history. A lymph node biopsy showed malignant tumor comprising of lymphocytes, histiocytes, eosinophils, atypical histiocytes and Reed Sternberg cells. On immunohistochemistry, atypical histiocytes and Reed Sternberg cells were positive for CD-15 and CD-30. A PET-CT scan [Fig.1] showed mediastinal lymphadenopathy. Patient was diagnosed as a case of Hodgkin’s lymphoma stage III-B, mixed cellularity type. Patient was given six cycles of chemotherapy with adriamycin (doxorubicin), bleomycin, vinblastin and dacarbazine (ABVD), achieving complete remission. A repeat PET-CT scan after 5 months, revealed no evidence of active disease. Patient remained asymptomatic for next 2 years after which he developed ataxia, dysarthria, seizures and altered sensorium. An MRI brain [Fig.2] showed a space-occupying lesion in the posterior fossa in the midline with significant adjoining edema resulting into obstructive dilatation of lateral and 3rd ventricles. CSF was negative for malignant cells. Additional workup with PET-CT scan whole body revealed intensely fludeoxyglucose (FDG) avid homogeneously enhancing rounded soft tissue mass lesion in the infratentorial brain parenchyma. There was no scan evidence of FDG avid disease in rest of the body surveyed. A neurosurgery opinion was taken and craniotomy with decompression was done. Histopathology of biopsy showed infiltration of brain tissue by malignant cells comprising of lymphocytes, plasma cells, eosinophils, atypical histiocytes, and Reed Sternberg cells. Reed Sternberg cells stained positive for CD-30. Three weeks after surgery an external beam radiotherapy (EBRT) to brain was given. Patient received EBRT to brain to a dose of 54 Gy/ 27 fractions to 90-95% isodense curve, whole brain technique 40 Gy/ 20 fractions initially followed by boost 14 Gy/ 7 fractions with IMRT technique. Following surgery and radiotherapy patient remained asymptomatic for next 9 months after which he presented with cervical lymphadenopathy. A small lymph node biopsy showed proliferation of large number of uninucleate and binucleate Reed Sternberg cells with small number of eosinophils. A further work up with PET-CT scan [Fig.3] showed resolution of previous cerebellar lesion and was suggestive of bilateral cervical and para-aortic lymphadenopathy [Fig.4]. Patient received six cycles of chemotherapy with ifosfamide, etoposide, mitoxantrone (MINE regimen) and intrathecal methotrexate. Last PET-CT scan showed no evidence of active disease. On last follow-up patient remained without evidence of either CNS or systemic Hodgkin’s lymphoma relapse.
CNS involvement by Hodgkin’s lymphoma is a serious complication that may occur in patients who are apparently in remission as was our case. Most of the evidence regarding CNS involvement in Hodgkin’s lymphoma comes from small case reports rather than the large series of patients; therefore, there is not enough evidence to start any treatment protocol [
2-
4].
The mechanism of brain spread is either through direct tumor extension or through meningeal involvement, or haematogenous spread [
5,6]. Hodgkin’s lymphoma can occur in various anatomical sites within the CNS. Ashby et al. found dural involvement more common than parenchymal lesions [
7]. Most lesions in intracerebral Hodgkin’s lymphoma have been supratentorial and only few infratentorial are reported, as is our patient. Nodular sclerosis and mixed cellularity are the most common histological subtypes of HL affecting the CNS [
3,
4,
8]. Presenting symptoms of CNS Hodgkin’s lymphoma can include pain, sensory impairment, weakness, papilloedema, ataxia, coma and seizures [
3,
8]. This depends on the part of brain involved, as in our patient cerebellar involvement lead to the symptoms of dysarthria, ataxia, seizures and altered sensorium.
Patients with CNS Hodgkin’s lymphoma may respond well to therapy. Gerstner et al. [
9] showed 69% overall response rate, with 56% achieving complete response. The treatment options in CNS Hodgkin’s lymphoma include surgery, radiation or chemotherapy alone or in combination. Corticosteroids can lead to rapid tumor regression. As a general rule such medication should be withheld prior to diagnostic biopsy in a clinically stable patient, however, patients with seizures, altered mental status, papilloedema or other evidence of significant mass effect, pre-biopsy corticosteroids may be necessary as in our case. A surgical approach should be considered at first to obtain histological confirmation. Our patient was treated with surgical excision followed by radiotherapy with good tolerance and satisfactory results. As our patient did not show any evidence of systemic Hodgkin’s disease at that time, hence no systemic chemotherapy was given.
To conclude, the presence of intracranial metastasis of Hodgkin’s lymphoma is an odd event in the course of disease and generally leads to adverse outcome. Due to lack of multicentric trials no universally accepted standard treatment option is available, however, an aggressive approach with surgery followed by chemo-radiation appears to be the best option.
References
- Re D, Fuchs M, Schober T, Engert A, Diehl A. CNS involvement in Hodgkin’s lymphoma. J Clin Oncol. 2007;25:3182.
- Baigi j, Mackenzie RG, Lim MS, Sapp M, Berinstein N. Primary Hodgkin’s Disease of CNS in an immunocompetent patient: A case study and review of literature. Neuro Oncol. 2000;2:239-243.
- Morawa E, Ragam A, Sirota R, Nabhan C. Hodgkin’s Lymphoma involving CNS. J Clin Oncol. 2007;11:1437-1438.
- Nakayama H, Tokuye K, Kagami Y, Sumi M, Murayama S,. Kawashima M, et al. Brain involvement in Hodgkin’s disease; case report and review of literature. Radiat Med. 2000;18:205-208.
- Ramirez C, Reyns N, Ayachi M, Blond S. Isolated intracranial relapse in previously treated Hodgkin’s disease. Rev Neurol (Paris) 2009; doi: 10.1016/j.neurol.2009.01.043.
- Hadadi K, Sifat H, et al. Intracranial Hodgkins Disease: case report. Cancer Radiother. 2002;6:285-288.
- Ashby MA, Barber PC, Holmes AE, Freer CE, Collins RD. Primary Intracranial Hodgkin’s disease: a case report and discussion. Am J Surg Patholog. 1988;12(4):294-299.
- Chim CS, Shek TW, Liang R. Unusual features of Hodgkin’s disease. Case 2: meningeal relapse in Hodgkin’s disease. J Clin Oncol. 2000;18(5):1150-1155.
- Gerstner ER, Abrey LE, Schiff D, Ferreri AJ, Lister A, Montoto S, et al. CNS Hodgkin’s lymphoma. Blood. 2008;112:1658-1661.