|
|
|
|
|
Segmental Rupture Bilateral Tendoachilles
|
|
|
Vipin Sharma, Abhimanyu Virmani, Bhanu Awasthi, Surjeet Singh, Manav Gupta, Punit Katoch
Department of Orthopaedics, Dr. Rajendra Prasad Government Medical College, Kangra, Himachal Pradesh-176001, India. |
|
|
|
|
|
Corresponding Author:
|
Dr. Vipin Sharma
Email: vipinsh_hp@rediffmail.com
|
|
|
|
|
|
|
|
|
Received:
09-JUL-2016 |
Accepted:
04-OCT-2016 |
Published Online:
15-NOV-2016 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Local steroids in tendoachillitis are frequently used to provide short term relief to the patient, an advantage that is closely associated with increased risk of tendon rupture. Here we are reporting a rare case of bilateral tendoachilles (TA) rupture in a patient following steroid injections for tendoachillitis. The open technique was used for surgical repair.
|
|
|
|
|
|
Keywords :
|
Achilles Tendon, Humans, Risk, Rupture, Tendon Injuries.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffa46b12000000f100000001001300 6go6ckt5b5idvals|685 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Although reported as a rare injury in past, tendoachilles rupture has emerged with increasing frequency almost upto 40% of all tendon ruptures. However, spontaneous bilateral Achilles tendon ruptures are a very uncommon occurrence [1]. Many risk factors like chronic pain, previous achilles tendon rupture and flouroquinolones have been identified but local injectable corticosteroids mostly given to alleviate pain of tendoachillitis have emerged as a major risk factor [2]. Very few cases of steroid induced spontaneous rupture of tendoachilles have been reported so far. The present case report is an attempt to highlight near fatal complication of spontaneous TA rupture following local steroid injection.
Case Report
A forty seven year old healthy male, bus driver by profession, developed sudden sharp pain in posterior aspect of both ankles in the region of Achilles tendon. There was no antecedent history of trauma. The pain was sudden in onset, high intensity, continuous and aggravated on walking. He was managed by local steroid injections in past by medical practioner and presented to us two months later with difficulty in ambulation and loss of plantar flexion power in both feet. Consent for examination, investigation and subsequent management was taken from the parents of the patient.
On clinical examination there was lump on the posterior aspect of both ankles. Deep palpation of the area revealed bilateral defect in the region of tendo Achilles [Fig.1]. Simmonds test was positive on both sides. Active plantar flexion movements at ankle were not demonstrable. The diagnosis was confirmed on MRI and planning done as operative management of the bilateral rupture.

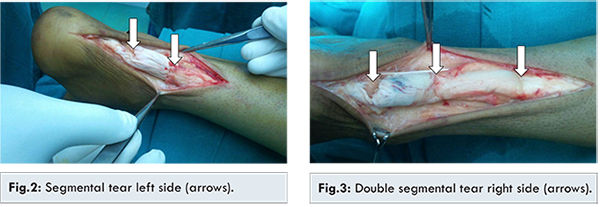
After appropriate anesthesia patient was taken in prone position. Posterio-medial incision was given bilaterally overlying tendoachilles. Per-operatively a segmental tear was noted on left side. The lower limit of the tear was 2.5 cm from the tendoachillis insertion and the upper limit was 5 cm from the insertion [Fig.2]. While on right side a double segmental tear was noted, the lower limit of the tear was 2.5 cm from the insertion, the upper limit of the tear was 10 cm from the insertion, and the middle tear was 6 cm from the insertion of the tendon [Fig.3]. Bilateral tendoachilles tendon repair was done using Ethibond sutures with modified Kessler’s technique on both proximal and distal part of the ruptured segment. Tendon ends could be approximated without much difficulty. The wound healed and the sutures were removed two weeks after surgery. Patient was in plaster immobilisation for six weeks. Physiotherapy was started six weeks after the procedure. A follow-up ultrasound done at six months of repair confirmed the healing of the TA tendon on both the sides. Patient has been in our follow up for more than a year with no complications, full range of ankle movements, pain free ambulation and ability to stand on tip toes.
Non-operative and operative methods have been mentioned in literature for treatment of TA rupture. The management options (non-operative vs operative) are chosen based on patient’s life style and demand, keeping in view benefits and risks assessment of each procedure. While conservative management may lead to healing with scar tissue, triceps surae contracture leading to its shorter functional length; operative management allows for primary healing, length restoration and maximum isokinetic strength of Achilles tendon.
Open repair of Achilles tendon ruptures is better as re-rupture rates are less as compared with non-operative treatment, though there is higher risk of infections and wound problems [3,4]. Usually young and athletic individuals are managed by surgical option as their Achilles tendons are subjected to repetitive high demand activity while elderly patients are managed by conservative methods like plaster immobilisation [5,6]. Open surgical reconstruction is undertaken using a medial longitudinal approach in view of better visualization of the plantaris tendon, and minimal injury to sural nerve. Medial approach is preferred over midline incisions as there are higher rates of wound complications and adhesion [5,7]. Failed conservative treatment and re-rupture are managed by operative treatment [8,9]. Percutaneous approach has an advantage over open approach as the former has advantage of less incidence of wound breakdown and infection but is likely to injure sural nerve [3,10].
Our patient reported with a segmental bilateral TA rupture following local steroid injection which is an unusual and rare presentation. No studies are available highlighting management of bilateral segmental TA rupture. The present patient was managed by open surgical repair of both tendons. Middle aged but active in job he was managed operatively to improve healing and allow early rehabilitation. Conservative management in this case might have resulted in large healing time, healing by fibrosis, incomplete healing, higher re-rupture rates and delayed rehabilitation. Modified Kessler technique was used for repair at both ends of each segment. Per-operatively primary repair with Ethibond sutures and without any tendon augmentation was possible. A follow up ultrasound confirmed tendon healing and by six weeks patient was able to return to work and routine activities.
Conclusion
This case report highlights the unusual presentation of TA rupture which was bilateral and segmental, not so far reported in literature. It highlights the perils associated with steroid injection in patients of tendoachillitis and stresses need of open repair for better healing especially in segmental ruptures.
References
- Kelly M, Dodds M, Huntley JS, Robinson CM. Bilateral concurrent rupture of the Achilles tendon in the absence of risk factors. Hosp Med. 2004;65:310-331.
- Orava S, Hurme M, Leppilahti J. Bilateral Achilles tendon rupture: a report on two cases. Scand J Med Sci Sports. 1996;6:309-312.
- Khan RJ, Fick D, Keogh A, Crawford J, Brammar T, Parker M. Treatment of Acute Achilles tendon ruptures. A metaanalysis of randomized, controlled trials. JBJS[Am]. 2005;87(10):2202-2210.
- Schepsis AA, Jones H, Haas AL. Achilles tendon disorders in athletes. Am J Sports Med. 2002; 30(2):287-305.
- Keene JS. Tendon injuries of the foot and ankle. In: DeLee JC, Drez D, eds. Orthopaedic sports Medicine. Philadelphia, Pa: WB Saunders; 1994:1768-1805.
- Maffuli N, Longo UG, Maffuli GD, Khanna A, Denarvo V. Achilles tendon ruptures in elite athletes. Foot Ankle Int. 2011;32(1):9-15.
- Moore KL. Clinically oriented anatomy. 3rd ed. Philadelphia, Pa: Lippincott Williams &Wilkins; 1999.
- Carr AJ, Norris SH. The blood supply of the calcaneal tendon. J Bone Joint Surg Br. 1989;71(1):100-101.
- Kader D, Saxena A, Movin T, Maffuli N. Achilles tendinopathy: some aspects of basic science and clinical management. Br J Sports Med. 2002;36(4):239-249.
- Saltzman CL, Tearse DS. Achilles tendon injuries. J Am Acad Orthop Surg. 1998;6(5):316-325.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Sharma V, Virmani A, Awasthi B, Singh S, Gupta M, Katoch PSegmental Rupture Bilateral Tendoachilles.JCR 2016;6:531-533 |
|
Sharma V, Virmani A, Awasthi B, Singh S, Gupta M, Katoch PSegmental Rupture Bilateral Tendoachilles.JCR [serial online] 2016[cited 2026 Mar 6];6:531-533. Available from: http://www.casereports.in/articles/6/4/Segmental-Rupture-Bilateral-Tendoachilles.html |

|
|
|
|
|