Introduction
The ingestion of hair dye (Super-Vasmol-33TM) is in trend as a major source of suicidal poisoning next to pesticides because of its easy availability and low cost. It is highly toxic when taken by mouth and the outcome depends mainly on the early management [1-4]. Supervasmol 33® is a popular emulsion-based permanent hair dye, containing mainly paraphenylene-diamine (PPD) [3]. The effect of PPD when ingested is serious and includes cervicofacial edema, mucosal injury, respiratory distress, rhabdomyolysis, acute renal failure and myocardial injury. The characteristic chocolate brown colour of urine could be confirmative evidence of hair dye poisoning in an individual with the poisoning of PPD [2,3,5]. We herewith report a case of hair dye poisoning who developed cardiac arrest and was managed successfully in our critical care.
Case Report
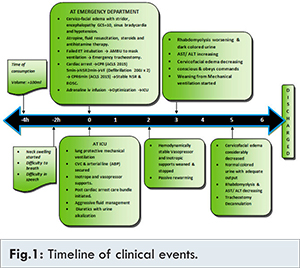
A 15-year-old female presented to the emergency department after ingestion of hair dye “SupervasmolTM with severe cervicofacial edema, respiratory failure and altered sensorium [Fig.1]. On examination she was semiconscious, restless with severe dyspnea and tachypnea (respiratory rate: 36/min) and tachycardia (heart rate: 130/min) with hypertension (blood pressure: 140/94 mmHg). In view of rapidly increasing cervicofacial swelling and respiratory distress endotracheal intubation was attempted, since the larynx could not be visualized, the procedure was quickly aborted and mask ventilation with Ambu started. However, ventilation was inadequate and patient started to desaturate and bradycardia ensued. Hence it was decided to perform emergency tracheostomy. Immediately following procedure, she developed worsening bradycardia followed by asystole. Cardiopulmonary resuscitation (CPR) started as per Advanced Cardiovascular Life Support (ACLS) guidelines and return of sinus rhythm with return of spontaneous circulation (ROSC) achieved within 5 minutes. But after 2 minutes, she developed ventricular fibrillation, for which she was defibrillated twice and CPR continued. After 6 minutes of CPR, sinus rhythm and ROSC achieved. She was started on adrenaline infusion and shifted to intensive care unit (ICU).
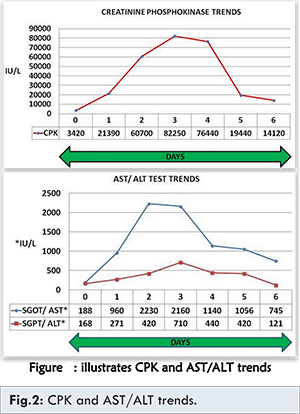
Her initial investigations showed, haemoglobin: 8.6 gm% and total counts: 17000/mm3. Her liver function tests were deranged with aspartate transaminase (AST): 188 IU/L, alanine transaminase (ALT): 168 IU/L. Creatine phosphokinase (CPK), lactate dehydrogenase (LDH) were high (3420 IU/L and 995 U/L respectively) and serum creatinine of 1.5 mg%. 2D echo (FATE) showed global hypokinesia and poor left ventricular function with ejection fraction: 20-25%. Her acid base gas analysis with 100% O2 revealed severe metabolic acidosis with hyperlactatemia (pH: 6.98, base excess of -17, bicarbonate of 14 meq/L and serum lactate of 74 mg%).
In the ICU, patient was started on lung protective mechanical ventilation. Aggressive fluid resuscitation was done. Central venous catheterization (CVC) was inserted to start vasopressor, inotropic supports and an arterial line secured for continuous ABP monitoring and blood sampling. Post-cardiac arrest care bundle was initiated (neuroprotective measures with therapeutic hypothermia, 34°C for 24 hours). Next 3 days, patient continued to be mechanically ventilated. She was hemodynamically stable, left ventricle contractility improved, vasopressor and inotropic requirements weaned and stopped on day 2, she was gradually rewarmed passively from 2nd day. Her cervicofacial edema decreased but liver injury and rhabdomyolysis worsened [Fig.2] and passed dark coloured urine for which she was managed with aggressive fluid therapy and forced diuresis with urine alkalization.
Subsequently, her cervicofacial edema considerably decreased. Liver injury, rhabdomyolysis were resolving and urine output was adequate with normal colour on 4th day. She was gradually weaned off from ventilator and tracheostomy decannulated on 5th day and later sent to ward on 6th day.
Discussion
Consumption of hair dye as a deliberate means of self-harm has been reported from different regions in India [1,2]. Rural poor, particularly young women are the common subjects for whom this agent is inexpensive and easily available [1,3,4]. Supervasmol 33® is a popular emulsion-based permanent hair dye. The main component of hair dye causing toxicity is paraphenylenediamine (PPD). This compound has been found to cause angioneurotic edema, rhabdomyolysis and renal failure [3,5].
In our patient, the most marked presentation as has been described elsewhere in literature was present. In such cases, the cervicofacial edema can severe enough to cause respiratory distress, hypoxia, and necessitate an early and emergency intubation or tracheostomy, which is lifesaving. In our patient we had to perform emergency tracheostomy on presentation in the ED, as we could not intubate. In-hospital cardiac arrests are secondary to presumed acute respiratory compromise and/ or circulatory shock, with predictable progressive deterioration before the event. Excellent outcomes can occur after well-choreographed, high quality CPR with effective chest compressions, ventilation and early defibrillation [8,9]. In our patient, cardiac arrest was promptly recognized, high quality CPR was instituted and optimized and later shifted to ICU for post-cardiac arrest care.
Effective post-cardiac arrest care consists of identification and treatment of the precipitating cause of cardiac arrest combined with the assessment and mitigation of ischemia-reperfusion injury to multiple organ systems [10]. Benefit is possible with appropriate forms of early goal-directed therapy and achieving therapeutic hypothermia within the first few hours, followed by gradual rewarming and ensuring glycaemic control. Creation of a bundle that incorporates these various aspects of care would more likely ensure that most patients recover with optimal neurological function [11]. In our patient we strictly adhered to the post-cardiac arrest bundle for 24 hours with positive outcome.
Acute renal failure is a reported complication of PPD poisoning. It occurs due to a combination of hypovolemia, toxic injury and myoglobinuria. Rhabdomyolysis can also be severe and if associated with high CPK can have an adverse outcome [6,7]. Our patient, however, responded to aggressive fluid management, forced diuresis with urine alkalization, maintaining a urine output >200 ml/hour and improved without haemodialysis in spite of very high levels of CPK.
Conclusion
Diagnosis of hair dye poisoning requires a high index of suspicion, as the clinical features are quite distinctive. Early recognition and treatment is vital with special emphasis on airway management, particularly to perform emergency tracheostomy if required. In case of cardiac arrest, follow ACLS guidelines for CPR and strictly adhere to post-arrest care bundle. Aggressive fluid management and forced diuresis with urine alkalization will minimize the risk of acute kidney injury. Institution of appropriate therapy without delay results in better outcome, including in a rural critical care setting.
References
- Sampathkumar K, Yesudas S. Hair dye poisoning and the developing world. J Emerg Trauma Shock. 2009;2:129-131.
- Chrispal A, Begum A, Ramya I, Zachariah A. Hair Dye poisoning: An emerging problem in the tropics: An experience from a tertiary care hospital in South India. Trop Doct. 2010; 40:100-103.
- Praveen Kumar AS, Talari K, Dutta TK. Supervasmol hair dye poisoning. Toxicol Int. 2012;19:77-78.
- Mary Nirmala S, Ganesh R. Hair dye. An emerging suicidal agent: our experience. Otolaryngology Online Journal. 2012;2(2):1-11.
- Bhargava P, Matthew P. Hair dye poisoning. J Assoc Physicians India. 2007;55:871-872.
- Huerta-Alardin AL1, Varon J, Marik PE. Bench-to-bedside review: Rhabdomyolysis - an overview for clinicians. Crit Care. 2005;9(2):158-169.
- Khan FY. Rhabdomyolysis: a review of the literature. Neth J Med. 2009;67(9):272-283.
- Garg SK, Tiwari R, Ahlawat A. Hair dye poisoning: An unusual encounter. Indian J Crit Care Med. 2014;18(6):402-404.
- Steven L. Kronick, Kurz MC, Lin S, Dana P. 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015;132(suppl 2): S397-S413.
- Clifton W. Callaway. Post-cardiac arrest care: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015;132(suppl 2):S465-S482.
- Anantharaman V. The post-resuscitation bundle. Singapore Med J. 2011;52(8):607.