Introduction
Cholelithiasis involves presence of stones or concretions in lumen of gall bladder. Gall stones develop insidiously and may remain asymptomatic for decades. It may evolve in four stages: (i) lithogenic state (ii) asymptomatic gallstones (iii) symptomatic gallstones (iv) complicated cholelithiasis.
Complications associated with cholelithiasis are acute cholecystitis, chronic cholecystitis, choledocholithiasis, cholangitis, pancreatitis, gall bladder malignancy, Mirrizi’s syndrome and gall stone ileus. Gallstone ileus is a rare complication of gallstones that occurs in 0.5% of all cases of bowel obstruction and in up to 25% of cases of non-strangulated small-bowel obstruction in patients over 65 years of age [
1]. The formation of a fistula between the gallbladder and the duodenum may allow a gallstone to enter the intestinal tract. Cholecystoduodenal fistula are most frequent (75%), followed by cholecystocolic fistula (10-20%), and a variety of other types (5-15%). Spontaneous enterobiliary fistulas occur secondary to biliary disease and disease of adjacent structures [
2]. We report a case of small-bowel obstruction diagnosed preoperatively as gallstone ileus, discussing the diagnostic features of the disease and reviewing the literature.
Case Report
A 70-year-old male patient presented in outpatient department (OPD) with complaints of intermittent epigastric pain and bloating for past 3 months. On physical examination, abdomen was soft with mild tenderness in right hypochondrium. Patient was a known diabetic and hypertensive for 10 years, on medication. No other known comorbidities were present. There was no past history of any surgery.
Ultrasound (USG) abdomen revealed contracted gall bladder with dense posterior shadowing suggestive of cholelithiasis with chronic cholecystitis. The patient was admitted for elective cholecystectomy and preanaesthetic work up. One day after admission, the symptom worsened and he developed severe nausea, vomiting and abdominal pain. Upon examination, abdomen was moderately distended, tympanic and high-pitched bowel sounds were audible. Rectal examination was normal. Blood tests revealed an elevated total leukocyte count and unremarkable liver function test values. Fasting blood sugars were borderline elevated. Blood pressure was 130/82 mmHg. Renal function tests were normal.
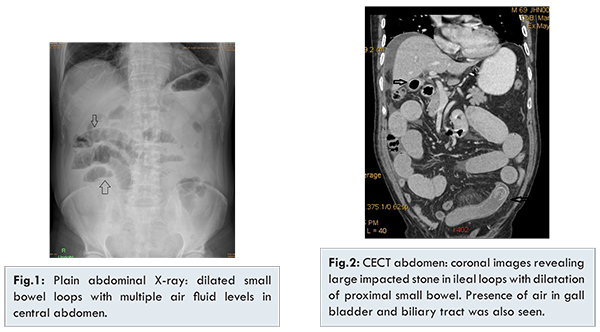
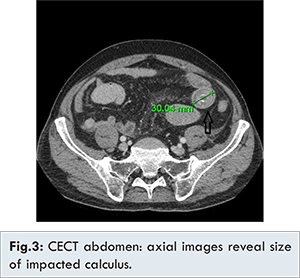
Plain radiographs of the abdomen done in erect and supine posture revealed dilated small bowel loops with multiple air fluid levels. Colonic gas shadows appeared normal and non-dilated [Fig.1]. A tentative diagnosis of small bowel obstruction was made. Oral intake was stopped and patient started on intravenous fluids and antibiotics. CECT abdomen was done on 128 slice dual energy GE CT scanner. Diluted ionic contrast was administered orally and intravenous contrast was given at rate of 2.5 ml/sec after delay of 70 sec. The images revealed multiple dilated fluid filled proximal small bowel loops. A large iso-hyperdense calculus measuring 30 mm was seen impacted in proximal ileal loop. CT also showed air in the gallbladder and biliary tracts- pneumobilia [Fig.2,3].
The final diagnosis of gall stone ileus was made. The patient was taken up for exploratory laparotomy during which enterolithotomy was done. Cholecystectomy and choledochoduodenal fistula repair was also done in same surgery. Patient complained of mild abdominal pain on post-operative day three. USG was done which revealed heteroechoic collection/hematoma in mesentery. It was treated conservatively and resolved spontaneously. Patient was discharged on postoperative day 12. Post discharge follow up was uneventful.
Discussion
Cholelithiasis is a common disease but is symptomatic only in 20%-30% of patients. It may present with vague pain, bloating and biliary colic as common symptoms [
3]. Our patient had initially presented in OPD with intermittent epigastric pain. Biliary-enteric fistula is the major pathologic mechanism of gallstone ileus. It is generally believed that peri-cholecystic inflammation after cholecystitis, as well as pressure necrosis by the gallstone against the biliary wall, may lead to formation of a biliary-enteric fistula. Fistula formation is a complication of 2% to 3% of all cases of cholelithiasis with associated episodes of cholecystitis [
4]. In our case the patient had cholelithiasis with chronic cholecystitis on first sonography.
A biliary enteric fistula provides a passage for large gallstones to enter the bowel which gets impacted and eventually cause gallstone ileus [
5]. The gallstone must be = 2-2.5 cm in diameter to cause obstruction [
6,
7,
8]. As shown by Reisner and Cohen, impaction of the stone can occur in any part of the bowel, i.e., the ileum (60.5% of cases), jejunum (16.1%), stomach (14.2%), colon (4.1%), and duodenum (3.5%). It can also be passed spontaneously (1.3%) [9]. It occurs most frequently in the terminal ileum and the ileocecal valve because of their narrow lumen and potentially less active peristalsis [
10]. The size of calculus in our case was 3.0 cm and it was seen impacted in proximal ileal loops.
The gallstone ileus is most commonly characterized by symptoms like nausea, vomiting and epigastric pain. Moreover, a small portion of patients may present with hematemesis secondary to duodenal erosions. Our patient was a known case of cholelithiasis with chronic cholecystitis and with sudden development of vomiting and abdominal pain - suspicion of gall stone ileus was high.
In 50% of cases the diagnosis is often only made at laparotomy. Lassandro et al. [
11] compared the clinical value of plain abdominal film, abdominal ultrasound and abdominal CT in diagnosing 27 cases of gallstone ileus, and found that the Rigler’s triad (mechanical small bowel obstruction, ectopic gallstone, and air in the biliary tree) presents 14.81% in plain abdominal film, 11.11% in abdominal US, and 77.78% in abdominal CT, respectively. CECT abdomen done in our patient had classical features of the triad as shown in Fig 2,3. The abdominal CT offers crucial evidence for diagnosis and appropriate management strategies of gallstone ileus.
The primary goal of treatment in gallstone ileus is early relief of intestinal obstruction and minimization of morbidity and mortality. Most reports indicate that stones smaller than 2.5 cm usually pass through spontaneously, so conservative treatment (decompression by nasogastric drainage) is conducted before a decision is made to remove the impacted stone by surgical means [
6]. The debate is still going on about the choice of procedure, whether a one stage or two-stage surgical procedure or enterolithotomy alone. The one-stage procedure includes enterolithotomy, cholecystectomy, and fistula repair in single sitting. The two stage procedure includes initial urgent enterolithotomy followed 4-6 weeks later by cholecystectomy and fistula closure. Our patient was treated with one stage procedure with enterolithotomy, cholecystectomy and fistula repair done in single surgery. The surgery was uneventful. Patient developed mesenteric hematoma during postoperative period which was managed conservatively.
Recently, laparoscopy-guided enterolitho-tomy has become the preferred surgical approach in treating gallstone ileus. The non-surgical treatment of gallstone ileus has been suggested, including endoscopic removal and shockwave lithotripsy depending upon the location of obstruction. The postoperative recurrence rate of gallstone ileus is 4.7% and only 10% of patients require secondary biliary surgery for recurrent biliary symptoms [
9,
12]. Some special types of such as Bouveret’s syndrome (stones impacting in the duodenum causing gastric outlet obstruction), and stones in the stomach or the colon are suitable for non-surgical therapeutic options in around 20% of the patients. For example laser lithotripsy in Bouveret’s syndrome [
13,
14] or extracorporal shock wave lithotripsy [
15] or even only endoscopic extraction [
8] may be a promising and fast therapeutic alternative.
Conclusion
In a patient with history of cholelithiasis with nausea, vomiting and abdominal pain, gallstone ileus must be considered as a differential diagnosis. Abdominal CT is usually the preferred diagnostic modality because of its rapid diagnosis and high resolution. The surgical management by enterolithotomy alone or enterolithotomy plus cholecystectomy and fistula repair are safe with marginal increased morbidity during one stage repair.
References
- Mohamed A, Bhat N. Gall Stone Ileus: A Rare Complication of Gallstone Disease. Case Report and Literature Review. The Internet Journal of Surgery. 2008 Volume 21 Number 1.
- Munghate A, Mittal S, Singh H, Garg A, Singh G, Sharma J. An uncommon cause of common presentation - Gall stone ileus: A case report and review of literature. Asian Journal of Medical Sciences. 2015;6(1):112-114.
- Berger MY, van der Velden JJ, Lijmer JG, de Kort H, Prins A and Bohnen AM. Abdominal symptoms: do they predict gallstones? A systematic review. Scand J Gastroenterol. 2000;35:70-76.
- Giese A, Zieren J, Winnekendonk G and Henning BF. Development of a duodenal gallstone ileus with gastric outlet obstruction (Bouveret syndrome) four months after successful treatment of symptomatic gallstone disease with cholecystitis and cholangitis: a case report. J Med Case Rep. 2010;4:376.
- Beltran MA, Csendes A, Cruces KS. The relationship of Mirizzi syndrome and cholecystoenteric fistula: validation of a modified classification. World J Surg. 2008, 32:2237-2243.
- Ihara E, Ochiai T, Yamamoto K, Kabemura T, Harada N. A case of gallstone ileus with a spontaneous evacuation. Am J Gastroenterol. 2002;97:1259-1260.
- Al-Obaid O. Gallstone ileus: A forgotten rare cause of intestinal obstruction. Saudi JGastroenterol. 2007;13:39-42.
- Xin-Zheng Dai, Guo-Qiang Li, Feng Zhang, Xue-Hao Wang, and Chuan-Yong Zhang. Gallstone ileus: Case report and literature review. World J Gastroenterol. 2013;19(33):5586-5589.
- Reisner RM, Cohen JR. Gallstone ileus: a review of 1001 reported cases. Am Surg. 1994;60:441-446.
- Gupta M, Goyal S, Singal R, Goyal R, Goyal SL, Mittal A. Gallstone ileus and jejunal perforation along with gangrenous bowel in a young patient: A case report. N Am J Med Sci. 2010;2:442-443.
- Lassandro F, Gagliardi N, Scuderi M, Pinto A, Gatta G, Mazzeo R. Gallstone ileus analysis of radiological findings in 27 patients. Eur J Radiol. 2004;50:23-29.
- Chou JW, Hsu CH, Liao KF, Lai HC, Cheng KS, Peng CY, et al. Gallstone ileus: Report of two cases and review of the literature. World J Gastroenterol. 2007;13(8):1295-1298.
- Tan YM, Wong WK, Ooi LL. A comparison of two surgical strategies for the emergency treatment of gallstone ileus. Singapore Med J. 2004;45:69-72.
- Maiss J, Hochberger J, Hahn EG, Lederer R, Schneider HT, Muehldorfer S. Successful laserlithotripsy in Bouveret’s syndrome using a new frequency doubled doublepulse Nd:YAG laser . Scan J Gastroenterol. 2004;39:791-794.
- Sackmann M, Holl J, Haerlin M, Sauerbruch T, Hoermann R, Heinkelein J, Paumgartner G. Gallstone ileus successfully treated by shock-wave lithotripsy. Dig Dis Sci. 1991;36:1794-1795.