6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff28621e0000004e07000001000900
6go6ckt5b5idvals|812
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Deltoid atrophy is often seen after brachial plexus trauma, isolated axillary nerve lesions, as a result of neurological impairment such as mononeuritis multiplex, or myalgic amotrophy. It may be associated with certain systemic diseases like poliomyelitis [1]. There are also some case reports of deltoid muscle dysfunction following intramuscular injections [2]. Duane’s retraction syndrome (DRS) is a congenital disorder with a limitation of abduction and/or adduction of the eye. In 70% of patients, DS is the only disorder the individual has. However, other conditions and syndromes have been associated with DS. These include malformation of the skeleton, ears, eyes, kidneys, and nervous system. DRS appears to be associated with an increasing number of musculo-skeletal abnormalities affecting mainly the upper limb [3-6]. It can be co-inherited with radial ray anomalies and hearing loss as an autosomal dominant trait, referred to as ‘Okihiro syndrome’ or ‘Duane’s Radial Ray syndrome’[7,8]. Radial dysplasia can range from hypoplasia of the thenar eminence with or without thumb abduction and apposition weakness, hypoplasia or absence of the thumb, and hypoplasia or complete absence of the radius and ulna. Associations with absent or hypoplastic upper limb muscles have been described in the Holt-Oram syndrome (associated with cardiac malformations) [6,9]. It has been documented in Wildervanck syndrome (fusion of neck vertebrae and hearing loss), Klippel-Feil (congenital fusion C2-C7) and in Poland’s syndrome (pectoralis muscle hypoplasia). Type 1 Duane’s syndrome is the most frequent form and can be associated with Klippel-Feil syndrome, thenar hypoplasia with or without absence of the thumb and first metacarpal, and deafness [3-5].
Numerous theories concerning the etiology and pathogenesis of DRS and its relation to the associated findings have been studied, but the exact mechanism is still being investigated. The most likely cause is a teratogenic stimulus during early gestation. Loci for Duane anomaly have been mapped to chromosomes 2q, 8q and 22 and lately mutations in SAL genes represent the first identified Duane Syndrome gene [7,10]. Although it may occasionally be seen as a familial feature, usually transmitted in autosomal dominant fashion, most patients with Duane’s related anomalies are sporadic cases.
Case Report
A 14 year old fit and healthy right handed boy presented to our paediatric orthopaedic clinic, having noticed a difference between his right and left shoulder in the rugby club changing room. His right shoulder looked ‘bony’ compared to the left [Fig.1,2]. He had no history of pain, although he did get some discomfort in his right shoulder when he had to write for longer than 30 minutes at school. His mother had a normal uncomplicated delivery at 35 weeks. He followed a standard vaccination program. Only one uneventful injection was given into the right deltoid. At the age of seven months his mother took him to the ophthalmologist because she noticed his inability to abduct his right eye. At that time the diagnosis of Duane’s retraction syndrome type 1 was made. No other abnormalities were noticed at that time. There was no history of shoulder or upper limb trauma, and no history of humeral osteomyelitis during his childhood.
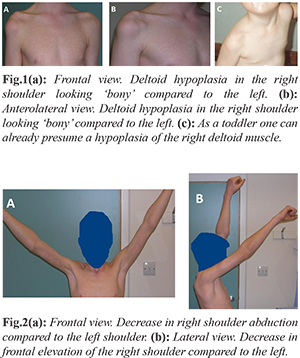
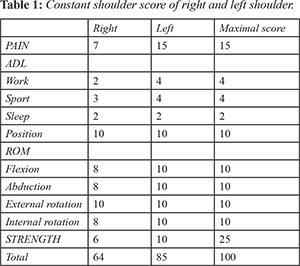
On pictures as a toddler, one can already appreciate a hypoplasia of the right deltoid muscle [Fig.1c]. There was no significant family history. Examination of his limbs was, with the exception of his right shoulder, completely normal. There was a slight decrease in shoulder abduction and forward elevation compared to the normal left shoulder (120° versus 150°), but otherwise the range of motions (ROM) between the two shoulders were similar. The overall Constant score was 64 on the right as compared with 85 on the left. The left side lost 15 points on strength as well on pain and ROM [Table 1]. X-rays of both shoulders, cervical spine and forearms did not show any bony pathology, but the hooked contouring of his right shoulder is quite remarkable [Fig. 3a].
The subacromial space was identical to the left shoulder. A MRI was performed and this clearly demonstrated the hypoplasia of the deltoid muscle, with some fibre-like muscle remnants, and hyperplasia of the rotator cuff, particularly the supraspinatus [Fig.3b,c]. An EMG was done to rule out an agenesis of the deltoid muscle or an axillary nerve palsy. This investigation demonstrated a normal insertional activity without spontaneously activity during rest nor any large polyphasic units or other changes suggestive of re-innervation.
Discussion
In this case the deltoid hypoplasia is of a non-traumatic aetiology. Most likely the hypoplasia was already present at birth but not yet visible because of the physiological amount of subcutaneous fat in the infant. Duane’s retraction syndrome has been associated with upper limb deformities in the hands [3-5,7], but, as far as we know, there are no reports of isolated unilateral ipsilateral deltoid hypoplasia in association with the syndrome. Although the term muscle fibrosis suggests that syndromes under this heading are primary disorders of muscle, evidence suggests that DRS may be a primary disorder of nerve innervation. Literature states that post-mortem studies did not identify large motor neurons at levels which the abducens nuclei normally occupy. It seems that some remaining muscle fibres are present but have a non-physiological function as seen on the EMG. One would need a biopsy of the remaining deltoid muscle fibres or an extensive DNA research to document the ongoing process. This patient is not significantly troubled by the lack of movement of his right shoulder. He is more concerned with the aesthetic appearance.
Although there are several procedures that could be considered to deal with his aesthetic concerns, it is the authors’ opinion that the risks of any such procedure outweigh the possible benefits. His rotator cuff is markedly hypertrophied. This raises the possibility that he may develop a premature impingement like syndrome with overstuffing of the sub-acromial space that may require surgery at an unusually young age.
Conclusion
It seems to be fair that children presenting with Duane’s retraction syndrome should be evaluated with X-rays of cervical spine and upper limbs for associated musculoskeletal abnormalities other than to the hand. Upper limb musculo-skeletal abnormalities appear to be associated with an increasing number of syndromes. If such abnormalities are found in the paediatric population, a full orthopaedic, medical and ophthalmologic assessment would seem to be essential.
Contributors: RH: manuscript writing, literature review, and patient management; AM: manuscript editing, literature review, and patient management; FJV: critical inputs into the manuscript, and patient management. RH will act as guarantor. All authors approved the final version of this manuscript.
Funding: None; Competing interests: None stated.
References
- Kumar K, Kapahtia NK. The pattern of muscle involvement in poliomyelitis of the upper limb. Int Orthop. 1986;10:11-15.
- Bodor M, Montalvo E. Vaccination-related shoulder dysfunction. Vaccine. 2007;25:585-587.
- Kargi SH, Koç F, Kargi E, Aköz T, Firat E. Bilateral Duane retraction syndrome associated with an extraordinary hand anomaly. Strabismus. 2003;11:157-162.
- Okihiro MM, Tasaki T, Nakano KK, Bennett BK. Duane syndrome and congenital upper-limb anomalies. A familial occurrence. Arch Neurol. 1977;34:174-179.
- Pernot C, Dupuis C, Gilgenkrantz S, Hueber JM. Holt-Oram syndrome and hand malformations associated with congenital heart disease. Arch Mal Coeur Vaiss. 1970;63:1428-1444.
- Ferrell RL, Jones B, Lucas RV. Simultaneous occurrence of the Holt-Oram and the Duane syndromes. J Pediatr. 1966;69:630-634.
- Al-Baradie R, Yamada K, St Hilaire C, Chan WM, Andrews C, McIntosh N, et al. Duane radial ray syndrome (Okihiro syndrome) maps to 20q13 and results from mutations in SALL4, a new member of the SAL family. Am J Hum Genet. 2002;71:1195-1199.
- Chun BB, Mazzoli RA, Raymond WR. Characteristics of Okihiro syndrome. J Pediatr Ophthalmol Strabismus. 2001;38:235-239.
- Cascos AS. Holt-Oram syndrome. Acta Paediatr Scand. 1967;56:313-317.
- Vincent C, Kalatzis V, Compain S, Levilliers J, Slim R, Graia F, et al. A proposed new contiguous gene syndrome on 8q consists of Branchio-Oto-Renal (BOR) syndrome, Duane syndrome, a dominant form of hydrocephalus and trapeze aplasia; implications for the mapping of the BOR gene. Hum Mol Genet. 1994;3:1859-1866.