6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff640a1d0000006607000001000400
6go6ckt5b5idvals|800
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Bell’s palsy is a common manifestation of isolated facial nerve palsy, where the patients present with acute onset unilateral facial paralysis. The etiology is unknown and the symptoms usually resolve over a period of six months [
1,
2]. The patient being described presented with features of Bell’s palsy but was found to have a pontine infarct, which is a rare scenario.
Case Report
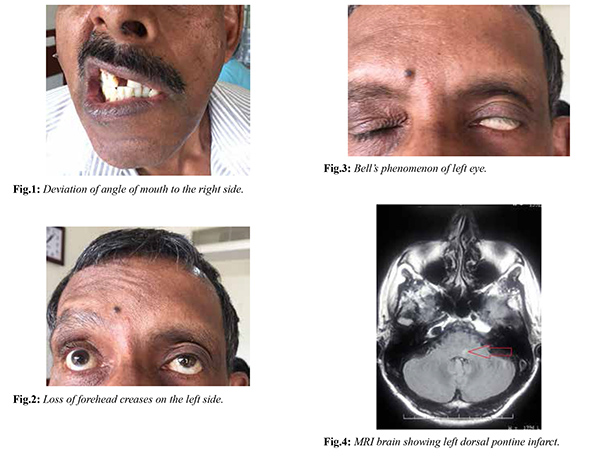
A 60 year old male, retired government employee, with no known co-morbidities presented with acute onset transient giddiness of one day duration. He is a smoker for the past 30 years (3-4 cigarettes/day). There was no associated dysarthria, ataxia, deafness, tinnitus or headache. The following day he noticed a deviation of angle of his mouth to the right side and difficulty in closing his left eye. He did not have any earache, rashes, limb weakness or sensory symptoms. There was no fever or symptoms of other systemic involvement.
On examination, he was conscious, oriented and afebrile. He had a regular pulse rate of 80/minute and blood pressure 160/100 mmHg. There was no mastoid tenderness, rashes or hearing disability. His neurological examination showed deviation of his angle of mouth to the right side [Fig.1], loss of naso-labial fold and forehead creases on the left side [Fig.2], inability to close his left eye and Bell’s phenomenon of left eye [Fig.3]. Other neurological and systemic examinations were normal. There was no carotid bruit. His blood investigations like complete blood count, renal and liver functions, thyroid profile, electrolytes and HbA1c were normal. Chest X-ray, ECG and echocardiogram were normal. A provisional diagnosis of Bell’s palsy was made. But considering the acute presentation of the patient along with hypertension, MRI brain was taken, which showed a tiny infarct involving the left dorsal aspect of the pons [Fig.4]. MR angiogram was normal.
He was started on perindopril (4 mg once daily), aspirin (75 mg once daily), clopidogrel (75 mg once daily) and atorvastatin (40 mg at night). His score on Modified Rankin Scale (mRS) and National Institutes of Health Stroke Scale (NIHSS) was 1 on presentation, and continued to be the same after a 30 days follow up. His House–Brackmann score improved from grade V to III within 30 days.
Discussion
The facial nerve (seventh cranial nerve) has two components; the motor and sensory roots which account for 70% and 30% of the fibres respectively. The motor root innervates the muscles of facial expression along with the muscles of scalp and ear [
3]. Bell’s palsy accounts for about 72% of facial palsies [
2], and frequently follows an immunization or viral infection [
3]. Other causes of peripheral facial weakness include motor neuron disease, Mobius syndrome, pontine lesions, cerebello-pontine angle mass lesions like acoustic neuroma, diabetes mellitus, HIV infection and Lyme’s disease [
3].
Around 7% of all ischemic strokes are due to pontine infarcts; and isolated pontine strokes are seen in about 15% of all posterior circulation infarcts [
4]. These infarcts are usually lacunar in size and involve mainly the basilar artery perforators [
5]. Pontine lesions presenting as facial palsy can be complicated. The facial nerve on the same side of the lesion may get damaged at the fascicular level, thereby causing a lower motor neuron lesion on that side. At the same time, if the upper motor neuron fibres to the opposite seventh nerve are damaged as they decussate, an upper motor seventh nerve lesion can be seen on the opposite side [
6].
With only a handful of cases being reported [
7,
8], isolated facial nerve palsy due to dorsal pontine infarct is a rare presentation. Our patient was not a known hypertensive and presented with features suggestive of typical Bell’s palsy. However, his acute presentation and elevated blood pressure raised the need to consider an imaging of the brain. MRI of the brain is an important imaging modality; and in this case picked up an infarct in the pons.
Conclusion
Isolated facial palsy following pontine infarct is a rare scenario, and can be easily misdiagnosed as Bell’s palsy. This case, therefore, highlights the need to consider MRI imaging of the brain in cases of isolated facial nerve palsy, especially when the presentation is acute, and in the setting of hypertension.
Contributors: UK: critical revision of manuscript and treating neurologist; RGM: concept and design of case report, reviewed the literature, manuscript preparation and treating physician. RGM will act as guarantor. Both authors approved the final version of the manuscript.
Funding: None; Competing interests: None stated.
References
- Bell’s palsy: Prognosis and treatment. Accessed on: http://www.uptodate.com/contents/bells-palsy-prognosis-and-treatment? source= search_result & selected Title=1%7E35. Accessed on August 15, 2017.
- Holland NJ, Weiner GM. Recent developments in Bell’s palsy. BMJ. 2004;329:553-557.
- Campbell WW. Pocket guide & toolkit to DeJong’s Neurologic Examination. 1st ed. Lippincott Williams & Wilkins, 2008. pp 119-126.
- Saia V, Pantoni L. Progressive stroke in pontine infarction. Acta Neurol Scand. 2009;120:213-215.
- Bassetti C, Barth A, Regli F. Isolated infarcts of the pons. Neurology. 1996;46:165-175.
- Patten J. Neurological differential diagnosis. 2nd ed. Springer, 2000. pp 172-173.
- Novy J, Michael P, Poncioni L, Carota A. Isolated nuclear facial palsy, a rare variant of pure motor lacunar stroke. Clin Neurol Neurosurg. 2008;110:420-421.
- Agarwal R, Manandhar L, Saluja P, Grandhi B. Pontine stroke presenting as isolated facial nerve palsy mimicking Bell’s palsy: a case report. Journal of Medical Case Reports. 2011;5:287.