6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffa488220000006d07000001000200
6go6ckt5b5idvals|860
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Darier disease, also known as dyskeratosis follicularis, is rare disorder of keratinization. Skin, nails and mucosa are primarily affected. It was first described in 1889 by Darier and White independently. With prevalence of 0.1 per million, it equally affects male and female [
1]. Characteristically, it manifests as warty, reddish brown papules and plaques primarily affecting seborrheic areas of skin on face, scalp, trunk and groin [
3]. Flexural Darier disease with lesions localized to flexures, is very rare [
3]. Cases with severe flexural involvement are commonly misdiagnosed as seborrheic dermatitis, pemphigus vegetans, pyoderma vegetans or Hailey-Hailey disease. We present a case of 40 year old female with hyper-keratotic plaques on flexural sites involving large skin folds.
Case Report
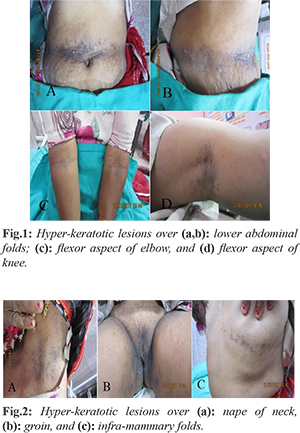
A 40 year old female presented with hyper-keratotic plaques of 2 years duration. She informed that initially these lesions were bullous with crust formation and after removal of crust verrucous plaque were formed. She was been treated accordingly but was not responding. The lesions were on flexural sites especially axillae and groin, nape of neck, submammary area, lower abdominal folds, ventral aspect of elbow and knee [Fig.1,2] and were associated with minimal itching. There was no occurrence of similar lesions in any other family member. On examination, she had hyper-keratotic verrucous lesions over large skin folds i.e. flexural areas with no signs of excoriation. Pits and longitudinal streaks were present on finger tips of both hands. Hair and oral mucosa were normal. The palms, soles, chest, back, scalp and face were spared.
Patient was subjected to battery of investigations including complete hemogram, renal function tests, liver function tests, electrolytes, lipid profile and imaging studies (chest X ray and ultrasound abdomen) all of which were within normal limits. Skin punch biopsy from lower abdominal fold was taken. The biopsy specimen was processed and stained with Hematoxylin-eosin (H&E) stain for histo-pathological examination.
On microscopic examination, sections showed hyperkeratosis, papillomatosis and dyskeratosis [Fig.3a,b] with formation of “corps ronds” [Fig.3c] and “grains” [Fig.3d]. There was suprabasal acantholysis with formation of lacunae or cleft [Fig.3a] and formation of villi which were lined by single layer of basal cells [Fig.3a,b]. Chronic inflammatory infiltrate were also seen in dermis. These features were consistent with Darier disease.
Discussion
In 1889, French dermatologist Jean Darier and American dermatologist James White independently gave first description of keratosis follicularis [
3]. The disease, now commonly called ‘Darier White disease’ is rare autosomal dominant genodermatosis caused by mutation in gene encoding ATP2A2 [
3] which regulates expression of sarcoplasmic reticulum calcium ATPase. Its mutation leads to abnormal intracellular calcium signaling. Eventually, there is loss of supra-basilar cell adhesion and apoptosis induction, histologically associated with acantholysis and dyskeratosis, respectively [
4,
5].
Classic lesions of Darier disease are localized to directly sun-exposed areas. Repeated irritation in form of heat and sweating exacerbates the disease and lesions which initially appear discrete papules, amalgamate to form large plaques. In its rare form, when lesions appear in flexural folds, they become hypertrophic and warty with increased propensity for secondary infection [
3]. The lesions are characteristically distributed in seborrheic areas, involving the scalp, forehead, ears, trunk and groin. Involvement of nails presents as nail dystrophy characterized by ‘V’ shaped notches at free edge, subungual hyperkeratosis and longitudinal ridges. Mucosal lesions are usually asymptomatic and clinically appear as multiple, normal colored or white, centrally depressed papules or ‘cobblestone lesions’ which predominantly affect palate [
3].
In 1992, Burge S and Wilkinson JD [3] first described the flexural variant of Darier disease with predominant involvement of flexures and minimal involvement of other commonly involved areas. Solely flexural localization is extremely rare [6]. Clinically, flexural Darier disease is commonly confused with seborrheic dermatitis, pemphigus vegetans, pyoderma vegetans or Hailey-Hailey disease. Histologically, it is hard to distinguish from diseases causing acantholysis and dyskeratosis like Grover’s disease. Darier disease can be readily distinguished from seborrheic dermatitis, clinically by acral and mucosal involvement or histologically by acantholysis. Pemphigus vegetans is late onset auto-immune disease that also produces acantholysis. In pyoderma vegetans, there is no acantholysis but neutrophilic infiltration is evident.
Hailey-Hailey disease is familial benign pemphigus which is characterized clinically by recurrent vesicular eruptions. Lesions are generally localized to the inter-triginous areas in form of soft, flat and moist vegetation along with painful fissures. Histo-pathologiocal examination can rule out these two conditions. In Hailey-Hailey disease, there is prominent acantholysis with larger supra-basilar separation, bullae formation and villous growth lined by single layer of basal cells. Characteristic dilapidated brick wall appearance in epidermis shows that despite extensive acantholysis there are few keratinocytes that are loosely attached with tonofilaments. In comparison, Darier disease show marked hyperkeratosis, papillomatosis and dyskeratosis in form of ‘corps ronds’ and ‘grains’; less acantholysis, less supra-basilar separation in form of lacunae formation and absence of dilapidated brick wall appearance in epidermis. Corps ronds are found in granular layer with central basophilic pyknotic nucleus surrounded by perinuclear halo. Grains are found in horny layer with elongated grain shape nuclei [7]. In Grover’s disease, also known as transient acantholytic dermatosis, focal itchy papulo-vesicular lesions appear transiently in response to sweating. These lesions are histologically similar to Darier disease but they are transient and do not tend to amalgamate.
In our case, presentation was atypical and unique. Patient was older than classical presentation in teens and lesions were atypically located involving large skin folds. Diagnosis was made by histo-pathological examination.
Conclusion
We reiterate through this case that clinico-pathological correlation is important for correct diagnosis of dematological lesions. Clinicians should be sensitized about atypical presentations of rare disorders like Darier disease. This case had involvement of all large skin folds and sparing of other parts. We conclude that although flexural involvement is uncommon but still Darier disease should be considered in the differential diagnosis of skin lesions present in flexural region.
Contributors: NS: manuscript writing, patient management; SRN: manuscript editing, patient management; NS will act as guarantor. All authors approved the final version of this manuscript.
Funding: None; Competing interests: None stated.
References
- Ferris T, Lamey PJ, Rennie JS. Darier’s disease: oral featuresand genetic aspects. Br Dent J. 1990;168:71-73.
- Cooper SM, Burge SM. Darier’s disease. Epidemiology, pathophysiology and management. Am J Clin Dermatol. 2003;4:97-105.
- Burge S, Wilkinson JD. Darier-White disease a review of the clinical features in 163 patients. J Am Acad Dermatol. 1992;27:40-50.
- Goldsmith LA, Baden HP. Darier-White disease (keratosis follicularis) and acrokeratosis verruciformis. In: Freedburg IM, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 6th edition. New york; Mcgraw-Hill, 2003:523.
- Hohl D, Mauro T, Gorog JP. Darier’s disease and Hailey-Hailey disease. In: Bolognia JL, Jorizzo JL, Rappini RP, editors. Dermatology. London: Mosby; 2003. pp. 823-833.
- Goh BK, Ang P, Goh CL. Darier disease in Singapore. Br J Dermatol. 2005;152: 284-288.
- Elder DE, Elenitsas R, et al. Lever’s Histopathology of the Skin; 11th ed. Philadelphia: Wolters Kluwer/ Lippincott Williams & Wilkins; 2014.