6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff243825000000e406000001000400
6go6ckt5b5idvals|893
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Coronary artery spasm, an intense vasoconstriction of coronary arteries that causes total or sub-total vessel occlusion presenting as acute coronary syndrome (ACS), can present with ST segment elevation myocardial infarction (STEMI), non-STEMI, or unstable angina. However, the prevalence of coronary spasm in patients with ACS remains unknown due to scarcity of data.
We are presenting two different patterns of coronary artery spasm: one focal and one diffuse, the first presenting as STEMI and the second as NSTEMI. These cases illustrate the need to incorporate routine intra-coronary injection of nitroglycerine to uncover coronary spasm in acute coronary syndrome (ASC), which can lead to either prevention of unnecessary stent insertion in the case of focal spasm, or to unmasking of a severe stenosis in the case of diffuse spasm, which would have gone undetected.
Case Report
Case 1
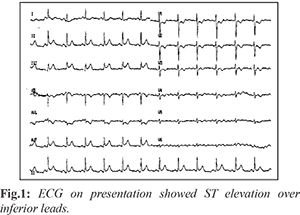
A 42 year-old gentleman, with a history of hypertension on dihydropyridine calcium channel blocker, heavy smoker, presented to our hospital with sudden onset severe retro-sternal chest pain which awakened him from sleep at 5:00 am. Electrocardiography (ECG) showed ST segment elevation in the inferior leads suggestive of acute inferior STEMI [Fig.1].
His full blood count, renal profile and random glucose were all within normal limits. Coronary angiogram was performed via right radial access. The diagnostic coronary angiogram showed a right dominant coronary artery giving rise to a large posterior descending artery (PDA) and a large postero-lateral (PL) branch, The PL branch had a proximal 60% stenosis followed by 90% focal stenosis [Fig.2]. After administration of 200 mcg intra-coronary nitroglycerine (NTG), both of these stenosis resolved completely [Fig.3] with resolution of inferior ST segment elevations, a finding consistent with spontaneous focal coronary spam mimicking a focal culprit stenosis, and this despite the patient being on oral amlodipine daily. The left system was completely normal.
The patient was treated medically with amlodipine, intravenous nitroglycerine which was switched to oral isosorbide mononitate, and counseled on smoking cessation.
Case 2
A 59 year-old gentleman presented with a history of anterior STEMI in 2006 treated at the time with primary percutaneous intervention (PCI) of the proximal left anterior descending (LAD) coronary artery and bare-metal stent insertion. He sustained an ACS with transient inferior ST elevations two weeks prior to this index admission, treated with PCI and drug-eluting stent insertion of a mid RCA hazy severe stenosis, presented with recurrent chest discomfort and a new serum troponin-T elevation. The patient had been on oral isosorbide mononitrate daily and was compliant with his dual anti-platelet regimen, His electrocardiogram didn’t show any ST-T wave changes [Fig.4].
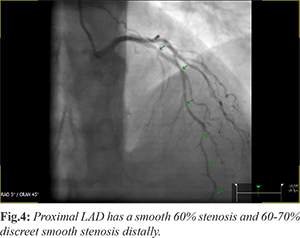
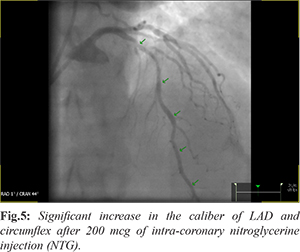
His full blood count and renal profile were all within normal limits. Coronary angiography was performed via right radial access. The initial diagnostic coronary angiogram showed what appeared to be a mild to moderate fixed stenosis in the proximal LAD proximal to the prior stent, with a moderate to severe focal stenosis more distally in the mid LAD [Fig.5]. The mid RCA stent was patent, and the circumflex had a moderate stenosis in its mid segment. After 200 mcg of intra-coronary nitroglycerine injection (NTG), there was a very significant increase in the caliber of LAD and left circumflex coronary artery, with total resolution of the distal LAD stenosis, consistent with definite spontaneous coronary spasm. This led to the unmasking of much more severe relative fixed stenosis in the proximal LAD and proximal circumflex.
The proximal LAD stenosis at proximal edge of prior stent had very positive fractional flow reserve measurement and was successfully treated with one DES. The intermediate proximal circumflex stenosis had a negative instantaneous wave free ratio/fractional flow reserve and no intervention was undertaken. The patient was discharged 24 hours post PCI on dual antiplatelet therapy, diltiazem 300 mg daily, isosorbide mononitrate high dose daily, and counseled on smoking cessation.
Discussion
Coronary artery spasm (CAS), an intense vasoconstriction of coronary arteries that causes total or sub-total vessel occlusion, plays an important role in myocardial ischemic syndromes including stable and unstable angina, acute myocardial infarction, and sudden cardiac death [
1].
Coronary artery vasospasm is the most common cause of non-obstructive lesions in acute coronary syndrome, the incidence of which is approximately 40-50% [
2]. Different ECG changes can appear during coronary artery spasm. The most important ECG change during a focal proximal coronary spasm in around 50% of cases is the appearance of peaked and symmetrical T waves that is followed, if the spasm persists, by progressive ST-segment elevation that last for a few minutes, and later progressively resolves [
3]. When coronary angiography is normal and spasm is still suspected, the standard method for diagnosing CAS relies on coronary angiography and provocative tests. However, coronary angiography is normal in about half of the cases [
3,
4]. Several cases have been reported of coronary spasms in the literature [
5,
6].
We are presenting two cases with two different patterns of coronary artery spam: one presenting as a focal lesion with STEMI and the other presenting with diffuse spasm of his entire left coronary tree. These cases of coronary spasm occurred despite the patients being on a calcium channel blocker in case number one, or on oral nitrates in case number two. The first case is a clear representation of focal coronary spasm causing inferior ST elevations on ECG and illustrates the critical role of intra-coronary nitroglycerin routine use in this setting before any “knee-jerk” stent implantation. The use of intra-coronary nitroglycerine should be attempted even in the inferior ST elevation setting, unless of course it is impossible secondary to right ventricular involvement and shock. In contrast, case number two illustrates the importance of intra-coronary nitroglycerin (NTG), first in uncovering spontaneous diffuse spasm in a patient with NSTEMI, despite being on oral vasodilators, and second, in uncovering the significant stable stenosis in the LAD which appeared non-significant in comparison to the reference vessel before nitroglycerin administration and confirmed by fractional flow reserve then stented successfully.
Conclusion
Although the use of intra-coronary nitroglycerin is very frequent during percutaneous intervention (PCI) for vessel sizing, its use should be standard of care in any patient with ACS, whether to ensure that fixed stenosis are not reversible, or to uncover “hidden” fixed stenosis when angiography only shows what appears to be relatively non-obstructive disease.
Contributors: AZ researched, gathered patient information, as well as wrote and revised the all the manuscript. AB assisted in guiding, editing, and providing valuable feedback throughout the project. AZ will act as study guarantor. Both authors approved the final version of this manuscript.
Funding: None; Competing interests: None stated.
References
- Hung MJ, Hu P, Hung MY. Coronary artery spasm: Review and update. Int J Med Sci. 2014;11:1161-1171.
- Onaka H, Hirota Y, Shimada S, Suzuki S, Kono T, Suzuki J, et al. Prognostic significance of the pattern of multivessel spasm in patients with variant angina. Jpn Circ J. 1999;63:509-513.
- de Luna AB, Cygankiewicz I, Baranchuk A, Fiol M, Birnbaum Y, Nikus K, et al. Prinzmetal angina: ECG changes and clinical considerations: A consensus paper. Ann Noninvasive Electrocardiol. 2014;19:442-453.
- Hung MJ, Hu P, Hung MY. Coronary artery spasm: Review and update. Int J Med Sci. 2014;11:1161-1171.
- Falsoleiman H, Bayani B, Dehghani M, Moohebati M, Rohani A. Global coronary arteries spasm in a young patient. ARYA Atheroscler. 2013;9:260-262.
- Liew CK, Leong WS. Coronary artery spasm (CAS) simulating inferior ST elevation myocardial infarction (STEMI). Med J Malaysia. 2012;67:108-110.