6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff28a3280000006907000001000300
6go6ckt5b5idvals|935
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Metastases to the temporal bone are exceedingly rare, representing <0.2% of all head and neck tumors. Gloria-Cruz et al. examined the prevalence of metastases to the temporal bone in 212 patients with primary non-disseminated malignant neoplasms. The colon was amongst the least common types, with only 2.1% of patients having it as their primary site of malignancy. Among histopathologic subtypes, adenocarcinoma was the most common type of malignancy found to metastasize to the temporal bone [1]. When delineating the metastatic areas within the temporal bone, the most common were the petrous apex, mastoid, internal auditory canal and middle ear. Presenting symptoms of temporal bone metastases vary but include hearing loss, vertigo or dizziness, facial weakness and tinnitus. It should however be noted that many patients are asymptomatic even when their disease burden is high [1].
Reports of metastatic colorectal adenocarcinoma to the temporal bone, as expected given the aforementioned information, are few, with only a handful of cases reported in the last 60 years [2-6]. Within this case report we describe a patient with known metastatic adenocarcinoma of the descending colon who presented with unilateral aural fullness, hearing loss and ataxia.
Case Report
A 64 year old female initially presented to her physician with abdominal pain and elevated liver enzymes. Ultrasound and subsequent biopsy of the liver revealed metastatic adenocarcinoma. Colonoscopy was performed and revealed the primary tumor within the descending colon. Further diagnostic workup at the time of presentation did not demonstrate any other metastatic deposits. The patient’s disease was deemed unresectable and she was initiated on palliative chemotherapy of FOLFIRI and bevacizumab, which she tolerated well.
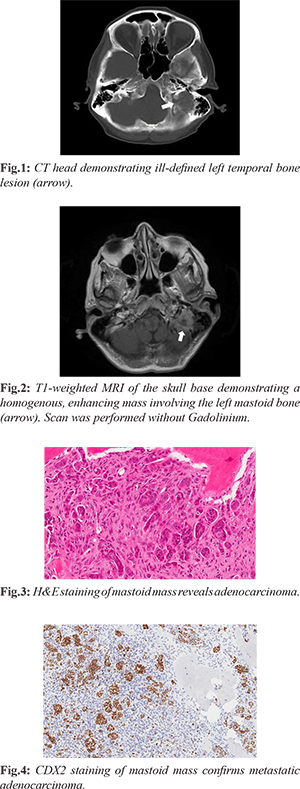
Approximately one year after initiating chemotherapy, the patient presented to her local emergency department with left sided aural fullness, hearing loss, ataxia and positional vertigo. The patient had no previous history of any otologic or vestibular conditions. A CT scan of the head [Fig.1] demonstrated an ill-defined, destructive mass within the left petrous bone. Subsequent MRI of the head revealed a 2.3 cm × 2.3 cm × 2.1 cm soft tissue mass in the left mastoid anterior to the sigmoid sinus and abutting the internal jugular vein [Fig.2]. Our initial assessment demonstrated right sided posterior semicircular canal benign paroxysmal positioning vertigo (BPPV) as the cause for the patient’s vertigo. Physical examination otherwise revealed a normal otoscopic examination and no facial weakness. The audiogram revealed normal low to mid frequency hearing on the right with a sloping moderate-severe sensorineural hearing loss. On the left, there was normal low to mid frequency hearing sloping to a severe high frequency sensorineural hearing loss. In addition, there was an elevated speech reception threshold on the left of 20 dB with 88% word recognition compared to 100% on the right. Given the concerning radiographic findings and the rarity of metastatic colon cancer to the temporal bone, the patient was offered biopsy and underwent a mastoidectomy with biopsy. Intra-operatively a fleshy mass was noted and pathologic analysis revealed metastatic colorectal adenocarcinoma, confirmed with CDX2 staining [Fig.3,4]. CK 20 staining was also performed and was consistent with metastatic colorectal adenocarcinoma.
On post-operative day two the patient developed a left sided facial paralysis, House-Brackmann grade four. Systemic corticosteroids were ineffective and the patient’s paralysis persisted. Over time the patient developed progressive dysphagia and weight loss. She was deemed unfit for further chemotherapy. Repeat MRI of the head two months after surgery demonstrated enlargement of the mass at 4.3 cm × 3.8 cm with compression of the sigmoid sinus and internal jugular vein [Fig.5]. In addition, there was significant narrowing of the jugular foramen and hypoglossal canal. Palliative radiotherapy to the temporal bone at 30 Gy over 10 fractions was performed.
The patient’s symptoms continued to progress and she was admitted to her local hospital for end of life care. She succumbed to her disease four months after the diagnosis of temporal bone metastasis.
Discussion
Metastases to the mastoid bone from adenocarcinoma of the colon are exceedingly rare, and few cases have ever been reported [2-6]. As such, relatively little is known regarding its presentation, natural history and optimal treatment methods. Various types of malignancies metastasize to the temporal bone including solid malignancies (lung and breast most commonly) [1,7] and hematologic malignancies such as leukemia [8]. The route of metastatic spread to the temporal bone is primarily hematologic; however, direct extension, meningeal carcinomatosis and leukemic infiltration can also occur [9]. A recent investigation by Song et al. described the clinical characteristics of temporal bone metastases. The authors found that the median duration from diagnosis of primary malignancy to temporal bone metastases was 22.5 months. In stark contrast, the median time to death from the diagnosis of temporal bone metastases was 3 months [10], highlighting the advanced stage of disease associated with this entity. In our patient, death occurred four months after the diagnosis of temporal bone metastasis. The largest series to date examining metastases to the temporal bone demonstrated that a significant proportion of patients are asymptomatic [1]. However, hearing loss, pain and facial paralysis have been described as presenting symptoms [10]. There can also be manifestations of other pathologies such as chronic otitis media, and temporal bone metastases can sometimes masquerade as more benign entities. Our patient coincidentally had BPPV, but of the contralateral ear, and it was successfully treated with the particle repositioning maneuver.
Diagnostic assessment for temporal bone metastases should include a detailed history and physical examination, audiogram, and CT/MRI of the temporal bone. Treatment of our patient’s metastasis was palliative using radiotherapy. This is reflective of the treatments that most individuals receive given the advanced stage of their disease at the time of diagnosis of temporal bone metastases [10].
Conclusion
Metastasis to the temporal bone is a rare clinical entity and represents a very small percentage of head and neck tumors. Patients with temporal bone metastasis have a poor prognosis as they tend to have very advanced disease. Here we describe a patient with biopsy-proven metastatic adenocarcinoma of the descending colon to the mastoid bone, one of only a few such case reports in the literature to date. Treatment options for these patients are limited to attempts at systemic treatment and local radiation as surgery is high-risk and unlikely to yield significant clinical benefit. Presenting symptomology can overlap with other, more common pathologies and as such, it is important to consider temporal bone metastases in symptomatic individuals with a history of an advanced primary malignancy.
Contributors: NM & SH: Literature review, development of manuscript; BW: provided histopathological images, edited manuscript. LP provided radiographic images, oversaw development of manuscript, edited manuscript. NM will act as a study guarantor. All authors approved the final version of this manuscript.
Funding: None; Competing interests: None stated.
References
- Gloria-Cruz TI, Schachern PA, Paparella MM, Adams GL, Fulton SE. Metastases to temporal bones from primary non systemic malignant neoplasms. Arch Otolaryngol Head Neck Surg. 2000;126):209-214.
- Merrick Y. Metastatic colon adenocarcinoma of the middle ear. Arch Otol. 1983;238:103-105.
- Frisch CD, Breen JT, Duckworth EA, Sweeney AD. Colon cancer metastasis to the lateral skull base masquerading as mastoiditis. J Neurol Surg B. 2017;78 (S01):S1-S156.
- Levine PA, Ruah CB, Bohigian K, Vincent ME, Vaughan CW. Metastatic sigmoid colon adenocarcinoma to the temporal bone. Otol HN Surg. 1987;97:500-503.
- Hill BA, Kohut RI. Metastatic adenocarcinoma of the temporal bone. Arch Otol. 1976;102:568-571.
- Jorgensen M. Metastatic carcinoma of the temporal bone. J Laryn Otol. 1961;75:513-518.
- Streitman MJ, Sismanis A. Metastatic carcinoma of the temporal bone. Am J Otol. 1996;17:780-783.
- Aljafar HM, Alsuhibani SS, Alahmari MS, Alzahrani MA. Temporal bone metastasis as a sign of relapsing chronic lymphocytic leukemia. Saudi Med J. 2015;36:1233-1235.
- Berlinger NT, Koutroupas S, Adams G, Maisel R. Patterns of involvement of the temporal bone in metastatic and systemic malignancy. Laryngoscope. 1980;90:619-627.
- Song K, Park KW, Heo JH, Song IC, Park YH, Choi JW. Clinical characteristics of temporal bone metastases. Clin Exp Otol. 2019;12:27-32.