ciproxin 500 torrino ciproxin 500 torrino website
From the Department of Pathology,
Government Medical College, Haldwani, Nainital, Uttarakhand, India.
Corresponding Author:
Dr. Ghazala Rizvi
Email: ghazalarizvi1970@gmail.com
Abstract
A 32 year old female patient with a soft boggy mass in the left axilla was referred from the surgery clinic for fine needle aspiration with a provisional diagnosis of fat hypertrophy. Physical examination revealed a well defined mobile nodule within the mass. Cytological examination of the aspirated material and histopathological examination was consistent with fibroadenoma.
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffb47b01000000b200000001000100 6go6ckt5b5idvals|136 6go6ckt5b5idcol1|ID 6go6ckt5b5|2000F757Tab_Articles|Fulltext Supernumerary breast and ectopic breast occurs in 1-6% of the general population. Ectopic breast tissue (EBT) occurs along the milk lines, extending from the mid axilla to the medial groins [1]. The embryological analogue of the milk line is the milk ridge, which later undergoes complete atrophy except for short segments that remain in the pectoral region to give rise to normal breasts. Ectopic or supernumerary breast develop from portions of the milk ridges that fail to atrophy.
Ectopic breast tissue shows pathologic changes similar to normally positioned breast and is a marker of urologic malformations or urogenital malignancies [2]. Though ectopic breast tissue has been reported but a fibroadenoma developing in EBT is a rare entity. We report a case of 32 year old woman with a fibroadenoma in ectopic breast tissue in axilla.
Case Report
A 32 year old woman with a soft boggy mass in the left axilla for the past 6 months was referred for fine needle aspiration with a provisional diagnosis of fat hypertrophy. The patient had no personal or family history of breast cancer. Both the breasts and nipples were clinically normal. Physical examination revealed a firm nontender lump, freely mobile within soft boggy mass which was completely isolated from the breast. The subsequent general and systemic examination was normal. The cytological examination of the material obtained by needle aspiration from this lump revealed cluster of cohesive epithelial cells admixed with myoepithelial cells. A provisional cytological diagnosis of fibroadenoma with no malignant change was made. The surgical excision of the lump showed a whitish cut surface [Fig. 1]. The sections taken from the mass revealed ductules lined by cuboidal epithelial cells resting on myoepithelial cell layer surrounded by abundant loose fibrous tissue [Fig. 2]. The histopathological picture was similar to the conventional type of fibroadenoma arising in normal breast tissue.
 Fig.1: Gross appearance showing a well-defined solid, grayish white tumour.
Fig.1: Gross appearance showing a well-defined solid, grayish white tumour.
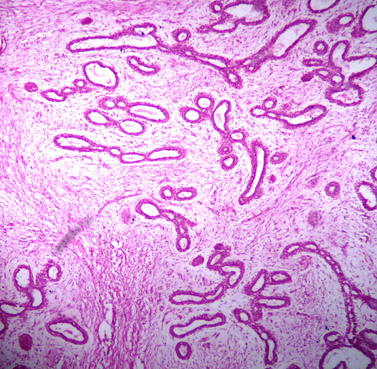 Fig.2: HPE shows predominantly intracanalicular pattern of fibroadenoma.
Discussion
During the early weeks of embryonic development the mammary milk lines extending from axillary region to groin develop from ectodermal thickenings along the sides of the embryo. Normally, entire embryological mammary ridges atrophy except for two segments in the pectoral region which later develop into the breast. Two hypotheses have been proposed on the embryogenesis of supernumerary breast. One attributes it to the failure of regression and displacement of the milk line, while the other believes that it develops from modified apocrine sweat glands [3]. A failure of the mammary ridge to involute may lead to ectopic breast tissue with (polythelia) or without (polymastia) a nipple/ areola complex [4]. Most instances of ectopic breast tissue occur along the milk line in the axilla [5], though they have been reported in areas other than the milk line region like the face, perineum and vulva [3,6]. Polythelia, in particular, has been associated with urinary anomalies such as supernumerary kidneys, renal agenesis and renal carcinomas. This can be partly explained by the parallel embryological development of mammary structures and genitourinary system [3,4]. Radiological examination to rule out urogenital malformations did not reveal any abnormality in our case. EBT demonstrates the hormonal effects similar to normal breast and is at a risk of developing breast diseases. It can undergo lactational changes during pregnancy and in the presence of nipple areolar complex can give rise to lactational secretions [4]. EBT harbours the risk of malignant transformation and in absence of nipple can delay the diagnosis of malignancy. Therefore such cases are associated with early and frequent metastasis resulting in poorer prognosis for the patient [7].
The clinical differential diagnosis for an ectopic breast tissue in axilla should include primary malignancies, benign cutaneous or subcutaneous tumors, infectious vascular lesions, as well as an axillary tail of Spence or a torn muscle belly. Even in patients presenting with axillary metastasis of an unknown primary tumor, ectopic breast tissue must be considered [8].
To conclude, any axillary mass should be treated with high index of suspicion keeping in mind ectopic breast tissue and all the pathologic changes of the breasts as early detection of a malignancy affects the prognosis of the patient.
References
Fig.2: HPE shows predominantly intracanalicular pattern of fibroadenoma.
Discussion
During the early weeks of embryonic development the mammary milk lines extending from axillary region to groin develop from ectodermal thickenings along the sides of the embryo. Normally, entire embryological mammary ridges atrophy except for two segments in the pectoral region which later develop into the breast. Two hypotheses have been proposed on the embryogenesis of supernumerary breast. One attributes it to the failure of regression and displacement of the milk line, while the other believes that it develops from modified apocrine sweat glands [3]. A failure of the mammary ridge to involute may lead to ectopic breast tissue with (polythelia) or without (polymastia) a nipple/ areola complex [4]. Most instances of ectopic breast tissue occur along the milk line in the axilla [5], though they have been reported in areas other than the milk line region like the face, perineum and vulva [3,6]. Polythelia, in particular, has been associated with urinary anomalies such as supernumerary kidneys, renal agenesis and renal carcinomas. This can be partly explained by the parallel embryological development of mammary structures and genitourinary system [3,4]. Radiological examination to rule out urogenital malformations did not reveal any abnormality in our case. EBT demonstrates the hormonal effects similar to normal breast and is at a risk of developing breast diseases. It can undergo lactational changes during pregnancy and in the presence of nipple areolar complex can give rise to lactational secretions [4]. EBT harbours the risk of malignant transformation and in absence of nipple can delay the diagnosis of malignancy. Therefore such cases are associated with early and frequent metastasis resulting in poorer prognosis for the patient [7].
The clinical differential diagnosis for an ectopic breast tissue in axilla should include primary malignancies, benign cutaneous or subcutaneous tumors, infectious vascular lesions, as well as an axillary tail of Spence or a torn muscle belly. Even in patients presenting with axillary metastasis of an unknown primary tumor, ectopic breast tissue must be considered [8].
To conclude, any axillary mass should be treated with high index of suspicion keeping in mind ectopic breast tissue and all the pathologic changes of the breasts as early detection of a malignancy affects the prognosis of the patient.
References
- De Cholnoky T. Supernumerary breast, Arch Surg 1939;39:926-941.
- Wise GJ, Roorda AK, Kalter R. Male breast disease. J Am Coll Surg 2005; 200:255-269.
- Aughesteen AA, Almasad JK, Al Muhtaseb MH. Fibroadenoma of the supernumerary breast of the axilla. Saudi Med J 2000; 21:587-589.
- Shin SJ, Sheik FS, Allenby PA, Rosen PP. Invasive secretory (Juvenile) carcinoma arising in ectopic breast tissue of the axilla. Arch Pathol Lab Med 2001; 125:1372-1375.
- Ciralik H, Bulbuloglu E, Arican O, Citil R. Fibroadenoma of ectopic breast of the axilla- a case report. Pol J Pathol 2006; 57: 209-211.
- Koltuksuz U, Aydin E. Supernumeray breast tissue, A case of pseudomamma on the face. J Pediat Surg 1997; 32:1377-1378.
- Roorda AK, Hansen JP, Rider JA, Huang S, Rider DL. Ectopic breast cancer, special treatment considerations in the postmenopausal patient. Breast J 2002; 8;286-289.
- Capobianco G, Spaliviero B, Dessole S, Rocca PC, Cherchi PL, Ambrosini G et al . Lymph node axillary metastasis from occult contralateral infiltrating lobular carcinoma arising in accessory breast: MRI diagnosis. Breast J, 2007;13: 305-307.
|