Manoj Kumar Gupta, Karsing Patiri1, Hari Shankar Pandey2
From the Department of Pathology,
Government Medical College, Ambedkar Nagar; Lady Hardinge Medical College, New Delhi1; Government Medical College, Haldwani2
Corresponding Author:
Dr. Manoj Kumar Gupta
Email: dr_manojgupta_1977_33@yahoo.co.in
Abstract
Fibrous dysplasia is a developmental anomaly of skeleton manifesting as defective osteoblastic differentiation and maturation. It is a nonheritable disorder of unknown aetiology. This report discusses a case of fibrous dysplasia at very unusual site i.e. fibula.
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff2493010000006200000001000300 6go6ckt5b5idvals|139 6go6ckt5b5idcol1|ID 6go6ckt5b5|2000F757Tab_Articles|Fulltext Fibrous dysplasia is a benign, abnormal growth of bone with an unknown aetiology where normal bone is replaced with fibrous bony tissue. Fibrous dysplasia has two clinical presentations, namely the monostotic and the polyostotic forms. The monostotic form constitutes about 70% of cases, having a predilection for the ribs and femur [1]. The polyostotic variety is usually present in developing children with unilateral presentation, skin hyperpigmentation, endocrine dysfunction and mostly affects craniofacial bones, ribs, femur and tibia. This case report discusses fibrous dysplasia occurring at an unusual site i.e. fibula and its differential diagnosis from other cartilaginous neoplasms.
Case Report
A 17-year-old male presented to our hospital with swelling in right leg since last 2 months. Swelling was accompanied by pain, was not increasing in size and was not preceded by history of trauma. Examination of his swelling showed nonpulsatile, hard swelling measuring 5 × 3 cm over right upper lateral aspect of fibula. There was no evidence of cutaneous hyperpigmentation or any other endocrinal defect. X-ray showed a radiolucent expansile metaphyseal lesion extending into proximal diaphysis and sparing of epiphysis in upper part of right fibula. There was evidence of few stippled and trabecular calcification with no obvious periosteal reaction or soft tissue swelling. Cortical integrity was maintained. Skeletal survey did not reveal any other abnormality.
Right fibulectomy revealed fusiform growth over upper part of fibula measuring 4 × 2.5 cm. Cut section showed expanded cortex with diffuse grayish white area and focal bluish gray translucent areas. On microscopic examination Chinese letter shaped immature bony trabeculae lacking a rim of osteoblasts was seen [Fig.1]. There was variable amount fibroblasts and spindle cell proliferation [Fig.2] with fibrocollageneous stroma and frequent areas of cartilaginous differentiation [Fig.3]. A histopathological diagnosis of fibrous dysplasia was made.
Discussion
Fibrous dysplasia occurs due to defective osteoblastic differentiation affecting the final maturation of the bone [2]. Although described as a congenital disorder of the bone, it usually manifests before the 3rd decade of life [3]. The age of our patient corresponded with the age described in the literature. Although fibrous dysplasia is a benign condition; in an unfavourable location like fibula it can cause considerable diagnostic and therapeutic problems. Complete surgical excision and immediate reconstruction have gained general acceptance to control fibrous dysplasia [4,5].
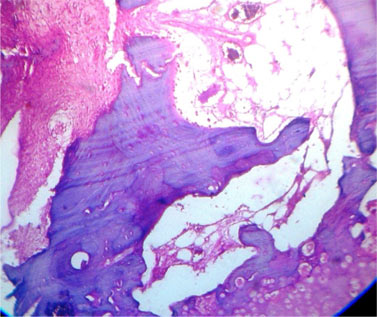 Fig.1: Chinese letter shaped immature bony trabeculae
Fig.1: Chinese letter shaped immature bony trabeculae
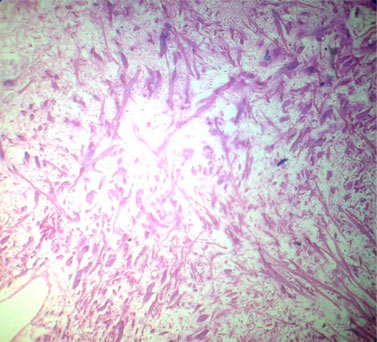 Fig.2: Fibroblasts and spindle cell proliferation
Fig.2: Fibroblasts and spindle cell proliferation
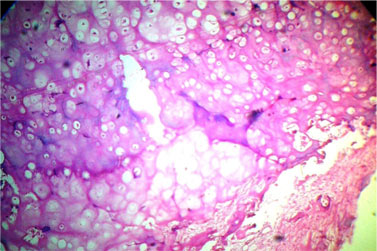 Fig.3: Cartilaginous differentiation
Fibrous dysplasia may show predominant fibrous & osseous area with infrequent cartilaginous areas. The cartilaginous areas widely vary from small foci to radiographically evident areas of extensive hyaline cartilage. Some authors have used the term ‘fibrocartilaginous dysplasia' (FCD) to describe fibrous dysplasia with extensive cartilaginous differentiation [6,7]. Sometimes the cartilaginous component is so extensive that it simulates a primary benign or malignant cartilaginous lesion. Thus differentiating FCD from other primary cartilaginous tumors is of significance in the management of these tumors.
Low-grade tumorous cartilage tissue juxtaposed against fibrous stroma may be mistaken as dedifferentiated chondrosarcoma. High grade spindle cells are frequently arranged in storiform pattern in dedifferentiated chondrosarcoma. Fibrosarcoma and malignant fibrous histiocytoma are frequent non-cartilaginous components of dedifferentiated chondrosarcoma [8,9]. Mesenchymal chondrosarcoma has its cartilage speckled throughout the tumour and mixed with a spindle or small-cell mesenchymal component. In fibrocartilaginous dysplasia, cellular areas of fibro-osseous stroma have to be searched for anaplasia before chondrosarcoma can be excluded from the differential diagnosis.
Other infrequent lesions that need to be considered in the differential diagnosis of fibrous dysplasia are desmoid tumour and low grade fibrosarcoma with enchondroma like nodules. These lesions have been termed as fibrocartilaginous mesenchymoma with low grade malignancy [10]. In these lesions, the histological appearance of the fibrous component is either an aggressive fibromatosis or a cellular fibroblastic lesion with minimal anaplasia that is consistent with low-grade fibrosarcoma [8,11]. The typical benign bony component of fibrous dysplasia is lacking.
Establishing the diagnosis of fibrous dysplasia is difficult due to nonspecific histological and radiological appearance which at times may result in poor characterization of the lesion. Therapeutic management depends on the course of tumour and the development of complications. This ranges from observation with serial radiological follow-up to medical treatment with systemic corticosteroid and surgical intervention [4]. In conclusion, monostotoic fibrous dysplasia of bone should be considered in the differential diagnosis of slowly progressive bony swellings in young adults.
References
Fig.3: Cartilaginous differentiation
Fibrous dysplasia may show predominant fibrous & osseous area with infrequent cartilaginous areas. The cartilaginous areas widely vary from small foci to radiographically evident areas of extensive hyaline cartilage. Some authors have used the term ‘fibrocartilaginous dysplasia' (FCD) to describe fibrous dysplasia with extensive cartilaginous differentiation [6,7]. Sometimes the cartilaginous component is so extensive that it simulates a primary benign or malignant cartilaginous lesion. Thus differentiating FCD from other primary cartilaginous tumors is of significance in the management of these tumors.
Low-grade tumorous cartilage tissue juxtaposed against fibrous stroma may be mistaken as dedifferentiated chondrosarcoma. High grade spindle cells are frequently arranged in storiform pattern in dedifferentiated chondrosarcoma. Fibrosarcoma and malignant fibrous histiocytoma are frequent non-cartilaginous components of dedifferentiated chondrosarcoma [8,9]. Mesenchymal chondrosarcoma has its cartilage speckled throughout the tumour and mixed with a spindle or small-cell mesenchymal component. In fibrocartilaginous dysplasia, cellular areas of fibro-osseous stroma have to be searched for anaplasia before chondrosarcoma can be excluded from the differential diagnosis.
Other infrequent lesions that need to be considered in the differential diagnosis of fibrous dysplasia are desmoid tumour and low grade fibrosarcoma with enchondroma like nodules. These lesions have been termed as fibrocartilaginous mesenchymoma with low grade malignancy [10]. In these lesions, the histological appearance of the fibrous component is either an aggressive fibromatosis or a cellular fibroblastic lesion with minimal anaplasia that is consistent with low-grade fibrosarcoma [8,11]. The typical benign bony component of fibrous dysplasia is lacking.
Establishing the diagnosis of fibrous dysplasia is difficult due to nonspecific histological and radiological appearance which at times may result in poor characterization of the lesion. Therapeutic management depends on the course of tumour and the development of complications. This ranges from observation with serial radiological follow-up to medical treatment with systemic corticosteroid and surgical intervention [4]. In conclusion, monostotoic fibrous dysplasia of bone should be considered in the differential diagnosis of slowly progressive bony swellings in young adults.
References
- Fletcher CDM, Unni KK, Mertens F. World Health Organization classification of tumors, Pathology and genetics of tumors of soft tissue and bone. IARC press, Lyon, 2002: pp. 341.
- Riminucci M, Fisher LW, Shenker A, Spiegel AM, Bianco P, Gehron Robey P. Fibrous dysplasia of bone in the McCune-Albright syndrome: abnormalities in bone formation. Am J Pathol 1997; 151:1587-1600.
- Hoffman S, Jacoway JR, Krolls SO. Fibrous dysplasia: Benign nonodontogenic tumors of the jaws. In: Seymour Hoffman (eds). Intraosseous and Periosteal Tumors of the Jaws. 2nd edition. Bethesda: Armed Forces Institute of Pathology; 1987:211-216.
- Chen YR, Noordhoff MS. Treatment of craniomaxillofacial fibrous dysplasia: how early and how extensive? Plast Reconstr Surg 1990;5: 835–842.
- Lustig LR, Holliday MJ, McCarthy EF, Nager GT. Fibrous dysplasia involving the skull base and temporal bone. Arch Otolaryngol Head Neck Surg 2001; 10: 1239–1247.
- Ishida T, Dorfman HD. Massive chondroid differentiation in fibrous dysplasia of bone (fibrocartilaginous dysplasia). Am J Surg Pathol 1993; 17:924-930.
- Vargas-Gonzalez R, Sanchez-Sosa S. Fiborcartilaginous dysplasia (Fibrous dysplasia with extensive cartilaginous differentiation). Pathology Oncology Research. 2006; 12:111-114.
- Frassica FV, Unni KK, Beabout JW, Sim FH. Dedifferentiated chondrosarcoma. A report of the clinicopathological features and treatment of seventy-eight cases. J Bone Joint Surg (Am) 1986; 68: 1197-1205.
- Johnson S, Tetu B, Ayala AG, Shawla SP. Chondrosarcoma with additional mesenchymal component (dedifferentiated chondrosarcoma). A clinicopathologic study of 26 cases. Cancer 1986;58:278-286.
- Campannaci M. Fibrous dysplasia. In: Bone and soft tissue tumors. Vienna and Bologna: Springer- Verlag and AuloGaggi Editore; 1990: pp. 391-417.
- Mirra JM. Fibrous dysplasia. In: Bone tumors. Clinical, radiologic and pathologic correlations. Philadelphia: Lea and Febirger; 1989: pp. 191-226.
|