Chayanika Pantola, Sanjay Kala1, P. K. Singh, Lubna Khan
From the Department of Pathology and General Surgery1,
GSVM Medical College, Kanpur, Uttar Pradesh, India.
Corresponding Author:
Dr Chayanika Pantola
Email: drchayanikakala@yahoo.com
Abstract
The inguinal lymph nodes are common site of metastasis from various organs. However, little is known about gallbladder carcinoma presenting as inguinal lymph node metastasis. We report a case of a primary gallbladder carcinoma with inguinal lymph node metastasis in a 65-year-old male. Clinically, our patient presented with enlarged inguinal lymph nodes without obvious signs and symptoms related to gallbladder carcinoma. Ultrasound abdomen suggested the possibility of a primary gall bladder carcinoma. Exact diagnoses could only be made after fine needle aspiration from gallbladder mass. A high index of suspicion, thorough clinical examination, cytopathological examination are essential to avoid misdiagnosis in such cases.
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffd4c9010000000b01000001000100 6go6ckt5b5idvals|147 6go6ckt5b5idcol1|ID 6go6ckt5b5|2000F757Tab_Articles|Fulltext Gallbladder carcinoma (GC) is the most frequent malignant neoplasm of the biliary tract and fifth most common malignant tumor of the gastrointestinal tract [1]. Advanced stage at diagnosis and nonspecific presentation leading to misdiagnosis makes its prognosis poor. The liver is the most commonly invaded organ by direct extension or metastasis, followed by regional lymph nodes [2,3]. Metastasis from gallbladder to inguinal lymph nodes, though known, is rare with only one report available in the English literature. Extra-abdominal metastasis could occur, but are rare [4,5]. This report describes the case of 65 year male of gallbladder carcinoma with initial presentation of enlarged inguinal lymph nodes.
Case Report
A 65 year male presented to surgery outpatient department with bilateral enlargement of inguinal lymph nodes. General physical examination revealed enlarged inguinal lymph nodes with largest node measures about 1.5x1.5 cm. An abdominal examination revealed no tenderness or abnormal mass. The results of complete blood count and serum chemistry panel on admission were normal. On the basis of these data bilateral fine needle aspiration was planned which revealed good cellularity with several small and large clusters of highly atypical cells forming acini at places with evidence of mucin production in few cells [Fig. 1 a, b]. The abdominal ultrasonography revealed the presence of a gall bladder mass lesion and enlargement of celiac, para-aortic and bilateral pelvic lymph node [Fig 2]. Ultrasound guided fine needle aspiration from gallbladder mass and largest mesenteric node revealed almost similar picture as that of inguinal nodes [Fig 1 c, d]. A final diagnosis of gall bladder adenocarcinoma with inguinal lymph node and intraabdominal metastasis was made. Patient was planned for chemotherapy and referred to oncosurgery.
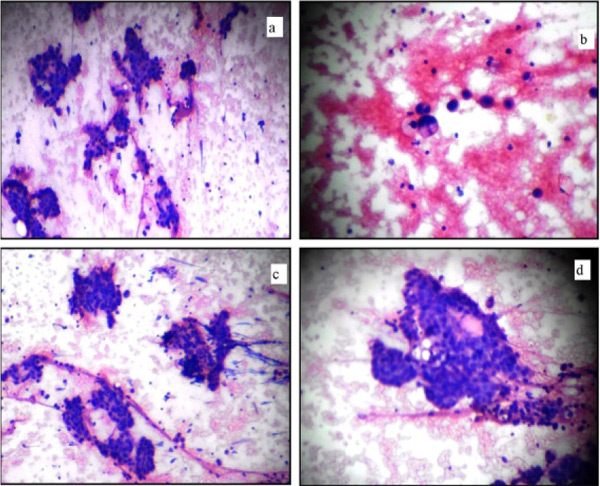 Figure 1
Figure 1
a. FNAC of inguinal node show atypical cells forming acini at places.
b. Atypical cell with evidence of mucin production.
c. FNAC of gall bladder mass also show atypical cells forming acini and short papillae at places.
d. FNAC of largest paraaortic lymph node node (100 x H& E).
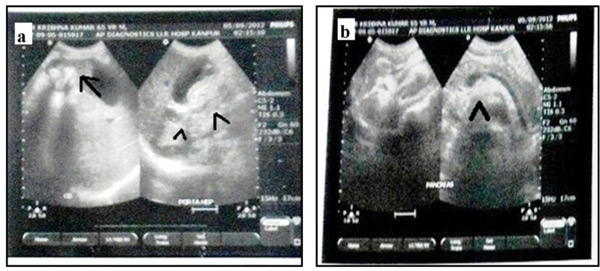 Figure 2
Figure 2
a) Ultrasonograph of abdomen show gallbladder mass (arrow) along with periportal lymph-node enlargement (arrow head).
b) Ultrasonograph of enlarged para-aortic lymph node (arrow head).
Discussion
Gall bladder cancer is a relatively uncommon disease in western world but common in Indian subcontinent [1]. Right hypochondrium pain is the most common symptom often mistaken for biliary colic or chronic cholecystitis. Other nonspecific presentations may be anorexia, indigestion of food, weight loos or upper abdominal discomfort. Patients with carcinoma of the gall bladder may have atypical presentations and unusual associations. The described atypical presentations of gall bladder carcinoma include empyema, acute cholecystitis, post-cholecystectomy benign biliary stricture, carcinoma of the head of pancreas, gastric outlet obstructions and liver abscess [6]. Unusual associations were common bile duct stones, left supraclavicular lymph node metastasis, Mirizzi's syndrome, inguinal lymph node metastasis and umbilical metastasis. The gall bladder carcinoma presenting with distant metastasis is rare and the rare sites include skin, bone and central nervous system, orbit and heart [4,7,8].
Gall bladder cancer generally disseminate by all route i.e. direct, lymphatic, hematogenous and peritoneal drop method. Direct invasion of liver followed by lymphatic spread is the commonest mode of spread[3]. Lymphatic metastasis from gall bladder goes to peripancreatic, celiac, mesenteric nodes. Shirai et al. reported that gallbladder lymph circulated though the pericholedochal lymph nodes to the posterosuperior pancreaticoduodenal lymph nodes, and interaoticoval lymph nodes [9]. Ito et al. have proposed three pathways of lymphatic drainage from the gallbladder: the cholecystoretropancreatic pathway, the cholecystoceliac pathway and the cholecystomesenteric pathway [10]. Reterograde spread from these node may explain the involvement of paraaortic and pelvic nodes and then retrograde spread to bilateral inguinal nodes as in our case.
Conclusion
Inguinal node is the common site for metastasis of malignancy of external genitalia, anorectal region and lower extremity. The gastrointestinal tract malignancies rarely metastasized to inguinal lymph nodes [11,12,13]. Inguinal lymph node metastasis should be added to the previously known sites of metastasis in gallbladder carcinoma. Knowledge of the extent to which inguinal lymphnode metastasis may be initial presentation of gallbladder tumor and its differentiating histological features may help in correct diagnosis and further management of the patient.
References
- Misra A, Misra S, Chaturvedi A, Srivastava PK. Orbital metastasis from gall bladder carcinoma. Br J Radiol 2002;75:72-73.
- Fahim RB, McDonald JR, Richards JC, Ferris DO. Carcinoma of the gallbladder: a study of its modes of spread. Ann Surg 1962;156: 114-124.
- Kokudo N, Makuuchi M, Natori T, Sakamoto Y, Yamamoto J, Seki M et al. Strategies for surgical treatment of gallbladder carcinoma based on information available before resection. Arch Surg 2003; 138: 741-750.
- Misra NC, Misra S, Chaturvedi A. Carcinoma of the gallbladder. In: Johnson CD, Taylor I, editors. Recent advances in surgery 20. London: Churchill Livingstone, 1997:69–87.
- Koo J, Wong J, Cheng FCY, Ong GB. Carcinoma of the gallbladder. Br J Surg 1981;68:161–165.
- Haribhakti SP, Awasthi S, Pradeep R, Kapoor VK, Kaushik SP. Carcinoma gallbladder :atypical presentations and unusual associations. Trop Gastroenterol 1997;18(1):32-34.
- Bardaji M, Roset F, Puig A, Badal J, Fernandez- Layos MJ. Cutaneous metastatic adenocarcinoma of gallbladder origin: report of a case and review of the literature. Hepatogastroenterology 1998;45: 930–931.
- Kawamata T, Kawamura H, Kubo O, Sasahara A, Yamazato M, Hori T. Central nervous system metastasis from gallbladder carcinoma mimicking a meningioma. Case illustration. J Neurosurg 1999; 6:1059.
- Shirai Y, Yoshida K, Tsukada K, Ohtani T, Muto T. Identification of the regional lymphatic system of the gallbladder by vital staining. Br J Surg 1992; 79: 659-662.
- Ito M, Mishima Y, Sato T. An anatomical study of the lymphatic drainage of the gallbladder. Surg Radiol Anat 1991; 13: 89-104.
- Wang PH, Lai CR, Wang TD, Chao KC, Ng HT, Yu KJ. Malignant mixed mesodermal tumor presenting as metastatic lymph node adenosquamous cell carcinoma: a case report. Zhonghua Yi Xue Za Zhi (Taipei). 1999 ;62(2):107-110.
- Ang D, Ng KY, Tan HK, Chung AY, Yew BS, Lee VK. Ovarian carcinoma presenting with isolated contralateral inguinal lymph node metastasis: a case report. Ann Acad Med Singapore. 2007;36(6):427-430.
- Vasso N, Agaimy A, Hohenberger W, Croner RS. Extraabdominal lymph node matastasis in gastrointestinal Stromal Tumours (GIST). J Gastrointestinal Surgery 2011;15(7):1232-1236.
|