AK Dawar, Kunal Gawri, Richa Dawar, Vikas Gupta
From the Department of Orthopaedics,
ESI Hospital, Okhla, New Delhi.
Corresponding Author:
Dr. A.K.Dawar
Email: dawar101@gmail.com
Abstract
We present a case of a patient with fibrolipomatous hamartoma of nerve. A 28-year-old man was admitted to our hospital complaining of swelling at lateral half of left hand for 7 years. Magnetic resonance imaging scans revealed Co-axial cable like appearance in axial sections and spaghetti like appearance in coronal sections. Excision of the mass revealed a large grayish white tumor under flexor retinaculum extending proximal to wrist joint with octopus like extensions in hand. Partial excision of tumor was done to prevent injury to nerves and flexor tendons. A pathologic diagnosis of fibrolipomatous hamartoma of nerve was made.
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffa4d1010000000d01000001000100 6go6ckt5b5idvals|148 6go6ckt5b5idcol1|ID 6go6ckt5b5|2000F757Tab_Articles|Fulltext Lipofibromatous hamartoma (LH) is a rare tumor like benign condition. It is thought to be congenital in origin [1,2]. Ever since its first report in 1953 by Mason [3], approximately 90 cases have been described in literature. Usually, upper limb nerves (mostly median nerve) are involved in first 3 decades of life with slight male preponderance. Mature fibrous and adipose cells infiltrate nerve tissue. Our case is unique in that contrary to normally adopted conservative approach, we resorted to surgical approach with satisfactory results.
Case Report
A 28-year-old man presented to our hospital for evaluation of a progressively increasing swelling of left hand for last 7 years. Our patient was a previously healthy man who had a blunt trauma to his hand 1 year prior to onset of swelling. The swelling started proximal to wrist joint gradually involving radial aspect of his left hand. While swelling was painful on dipping hand in cold water, the pain was not present during routine daily activities. Examination revealed, the soft subcutaneous non-tender swelling extending 6 cm proximal to wrist joint with involvement of thenar eminence, first introsseous space, volar aspect of thumb and ring finger upto proximal interphalangeal joint. There was no sensory deficit and wasting of hand muscles. General examination did not reveal any evidence of neurofibromatosis.
X rays showed a soft tissue mass in forearm and hand without evidence of bony hypertrophy or calcification.MRI report hinted at possibility of hemangioma due to appearance of tortuous voids in soft tissue mass. Since the swelling was interfering with his work, it was decided to debulk the tumor. The swelling was found to be greyish tumor 16x7.5x5 cm [Fig. 1] in size extending to hand through carpal tunnel. It was an octopus like mass with multiple linear extensions in all directions, and was not capsulated. Finger like extensions were found to be attached to under surface of skin of hand. The tumor was adherent to surrounding structures including flexor tendons and lumbricals but was not attached to median nerve. Sub-total excision of tumor was carried out without cutting transverse carpal ligament. A part of tumor extending to dorsal aspect of first introsseous space was not removed. Post-operatively, wound healed normally. However, he developed decreased sensations of index and middle fingers. Histopathology was reported as Lipomatous hamartoma [Fig. 2].
 Fig. 1: Gross excised specimen showing grayish white tumour.
Fig. 1: Gross excised specimen showing grayish white tumour.
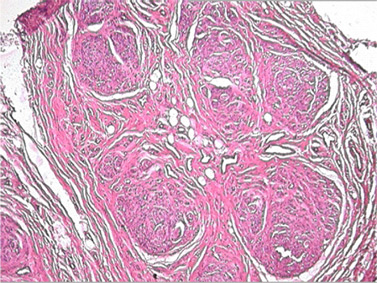 Fig. 2: Histopathology showing infiltration of nerve fascicles by mature adipose cells.
His one year follow up, has shown improved finger sensation with normal motor function of hand and fingers without any wasting of thenar muscles.
Discussion
Lipofibromatous hamartoma of nerve also known as neural fibrolipoma is rare tumor like condition. According to new WHO classification [4], it has been designated as nerve lipomatosis. Even though the etiology remains unknown, nerve hamartomas might be congenital in origin and usually manifest in first 3 decades of life. There is infiltration of fibrofatty tissue in and around nerve fibers and fascicles causing enlargement of nerve. Most commonly, it affects median nerve followed by radial, axillary, musculo-cutaneous, brachial plexus, cranial and plantar nerves. Usually there is minimal neurologic deficit, but symptoms of carpal tunnel syndrome may be there. It is associated with macrodactly in 1/3 cases [1].
MRI findings are pathognomic; co-axial cable like appearance in axial sections and spaghetti appearance in coronal sections [5]. In our case, classical features of LFH were reported [Figure 3,4]. MRI is also helpful in differentiating nerve hamartoma from neural lipoma, neurofibroma and malignant conditions [6,7].
Treatment of neural fibrolipoma is controversial. Most often “wait and watch approach “is applied. Total excision of tumor is not recommended for fear of causing sensory and motor deficit. However, excision of tumor involving cutaneous branches can be done [8,9]. Some authors perform neurolysis, decompression or intraneural microdissection of neoplastic elements [10]. Excision of median nerve in children has been successfully done due to Martin Gruber connections [11]. Debulking can be done, but it may compromise neurologic function. Due to rarity of this condition, controlled studies are not possible with respect to treatment modalities. Therefore, it is necessary to publish case reports of this condition so that surgeons can plan for the best treatment for their patients.
References
Fig. 2: Histopathology showing infiltration of nerve fascicles by mature adipose cells.
His one year follow up, has shown improved finger sensation with normal motor function of hand and fingers without any wasting of thenar muscles.
Discussion
Lipofibromatous hamartoma of nerve also known as neural fibrolipoma is rare tumor like condition. According to new WHO classification [4], it has been designated as nerve lipomatosis. Even though the etiology remains unknown, nerve hamartomas might be congenital in origin and usually manifest in first 3 decades of life. There is infiltration of fibrofatty tissue in and around nerve fibers and fascicles causing enlargement of nerve. Most commonly, it affects median nerve followed by radial, axillary, musculo-cutaneous, brachial plexus, cranial and plantar nerves. Usually there is minimal neurologic deficit, but symptoms of carpal tunnel syndrome may be there. It is associated with macrodactly in 1/3 cases [1].
MRI findings are pathognomic; co-axial cable like appearance in axial sections and spaghetti appearance in coronal sections [5]. In our case, classical features of LFH were reported [Figure 3,4]. MRI is also helpful in differentiating nerve hamartoma from neural lipoma, neurofibroma and malignant conditions [6,7].
Treatment of neural fibrolipoma is controversial. Most often “wait and watch approach “is applied. Total excision of tumor is not recommended for fear of causing sensory and motor deficit. However, excision of tumor involving cutaneous branches can be done [8,9]. Some authors perform neurolysis, decompression or intraneural microdissection of neoplastic elements [10]. Excision of median nerve in children has been successfully done due to Martin Gruber connections [11]. Debulking can be done, but it may compromise neurologic function. Due to rarity of this condition, controlled studies are not possible with respect to treatment modalities. Therefore, it is necessary to publish case reports of this condition so that surgeons can plan for the best treatment for their patients.
References
- Silverman TA, Enzinger FM. Fibrolipomatous hamartoma of nerve. A clinicopathologic analysis of 26 cases. Am J Surg Pathol 1985;9:7-14.
- Langa V, Posner MA, Steiner GE. Lipo?broma of the median nerve: a report of two cases. J Hand Surg [Br] 1987;12:221-223.
- Mason ML. Proceedings of the American Society for Surgery of the Hand: presentation of cases. J Bone Joint Surg Am 1953;35:273-275.
- Fletcher CDM, van den Berg E, Molenaar WM. Pleomorphic malignant fibrous histiocytoma/undifferentiated high grade pleomorphic sarcoma. In: Fletcher CDM, Unni K, Mertens F, (eds). World Health Organization Classification of Tumours. Pathology and Genetics of Tumours of Soft Tissue and Bone. Lyon, France: IARC Press; 2002. pp. 120–122.
- Maron E, Helms C. Fibrolipomatous hamartoma: pathognomonic on MR imaging. Skel Radiol 1999;28:260 –264.
- Nogueira A, Pena C, Martinez MJ, Sarasua JG, Madrigal B. Hyperostotic macrodactyly and lipo?bromatous hamartoma of the median nerve associated with carpal tunnel syndrome [review]. Chir Main 1999;18:261-271.
- Boren WL, Henry Jr RE, Wintch K. MR diagnosis of ?brolipomatous hamartoma of nerve: association with nerve territoryoriented macrodactyly (macrodystrophia lipomatosa). Skeletal Radiol. 1995;24:296-297.
- Amadio PC, Reiman HM, Dobyns JH. Lipo?bromatous hamartoma of nerve. J Hand Surg. [Am] 1988;13:67-75.
- Paletta FX, Senay Jr LC. Lipo?bromatous hamartoma of median nerve and ulnar nerve: surgical treatment. Plast Reconstr Surg. 1981;68:915-921.
- Terzis JK, Daniel RK, Williams HB, Spencer PS. Benign fatty tumors of the peripheral nerves. Ann Plast Surg. 1978;1:193-216.
- Bergman FO, Blom SE, Stenstrom SJ. Radical excision of a ?bro-fatty proliferation of the median nerve, with no neurological loss symptoms. Plast Reconstr Surg. 1970;46:375-380.
|