benadryl and pregnancy risks benadryl and pregnancy second trimester where to get abortion pill abortion rights read
From the Department of Surgery,
N.K.P.Salve Institute of Medical Sciences and Research Center,
Nagpur, Maharashtra, India.
Corresponding Author:
Dr. Diwakar Sahu
Email: diwakargmcbhopal@rediffmail.com
Abstract
Meckel's diverticulum is the most common congenital anomaly of the gastrointestinal tract with a complication risk of 4 – 6%. Enterolith formation is a rare complication of Meckel's diverticulum; rarely does a Meckel's diverticulum containing an enterolith, presents as a perforation in diverticulum and acute abdomen. Our case highlights one such unusual presentation in a patient presenting with abdominal pain.
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff4ce1010000000f01000001000e00 6go6ckt5b5idvals|152 6go6ckt5b5idcol1|ID 6go6ckt5b5|2000F757Tab_Articles|Fulltext Meckel's diverticulum was first described by Fabricius Hildanus in 1598. The name is derived from the German anatomist Johann Friedrich Meckel who described the embryological and pathological features in 1809 [1]. Meckel's diverticulum is the remnant of the prenatal Vitello-intestinal duct, occurring in approximately 2% of the population. It has risk of 4-6% to become symptomatic during lifetime and mainly presents with complications like acute gastrointestinal bleeding, intussusception, diverticulitis or perforation and obstruction, usually during adulthood [2].
Enterolith formation is a rare complication of Meckel's diverticulum. Meckel's diverticulum enterolith can cause intermittent abdominal pain, chronic gastrointestinal blood loss as well as diverticulitis, perforation or intestinal obstruction. Meckel’s diverticulum perforation due to enterolith is very rare and only few cases have been reported till date [3,4].
Case Report
A 60 year old male patient was admitted to our hospital with 3 day history of severe abdominal pain and vomiting with fever. Also, patient was a known case of diabetes with hypertension. She was tachycardic, tachypnoeic, and pyrexial. Abdominal examination revealed generalized distension and tenderness with preservation of bowel sounds. Laboratory data were all within normal limits including inflammatory response, liver function tests, and biliary enzymes.
Plain abdominal radiographs revealed no obvious perforation or obstruction and ultrasound abdomen showed edematous pancreas with minimal free fluid in pelvis. A CT scan of her abdomen demonstrated mild wall thickening of small bowel loops in lower abdomen with mild haziness in surrounding fat and enlarged lymph node with minimal free fluid [Fig.1]. As diagnostic dilemma still persisted, patient was posted for exploratory laparotomy. Intra operatively about 200 ml of pus was found with small bowel adhesion and inter bowel loop collection. Meckel’s diverticulum- 8 cm in length containing a large calculus of 3x4 cm lodged inside it was present 55 cm from ileo-cecal junction [Fig 2]. Apex of diverticulum was perforated with bowel contents oozing from it [Fig. 3]. Adjacent bowel was edematous and appendix was mildly inflamed for which appendectomy was done. Meckel’s diverticulum with adjacent bowel was resected and anastomosis done in double layer. Post operative course was uneventful and patient recovered well.
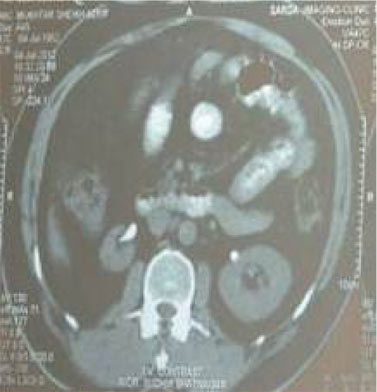 Fig.1: CT Scan showing enterolith between bowel loops
Fig.1: CT Scan showing enterolith between bowel loops
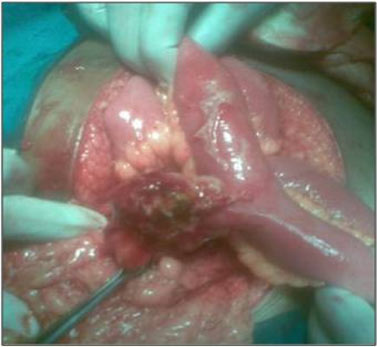 Fig.2: Meckel’s diverticulum with impacted enterolith
Fig.2: Meckel’s diverticulum with impacted enterolith
 Fig. 3: Specimen showing perforated Meckel’s diverticulum with enterolith and appendix
Discussion
Enteroliths in association with Meckel's diverticulum have been rarely described in literature. Authors of one study reviewed the records of 776 patients with Meckel diverticulum and found stones in only two patients while a study conducted at Armed Forces Institute of Pathology reported a much higher incidence in which 8 of 84 cases in 24 years contained stones [5,6] .
The alkalinity of the distal small bowel favours precipitation of mineral salts which along with pooling of intestinal content and inspissation leads to enterolith formation [7]. Stone formation in Meckel's diverticula occurs more commonly in diverticula that do not usually contain ectopic gastric mucosa [8]. Enteroliths originating from a Meckel's diverticulum have also been associated with intestinal perforation [7,9].
Accurate diagnosis of diverticular perforation due to enterolith impaction is generally demanding. In abdominal X-ray, radio-opaque Meckel's enteroliths can be visualized in 20-25% of the cases suggesting that Meckel's enteroliths should be included in the differential diagnosis of abdominal calcification [4]. However, small bowel contrast studies and imaging modalities such as CT scan have been considered more useful. Ileus or perforation due to Meckel's enterolith must be differentiated from gallstone enterolith, appendicolith, teratoma and calcified lymphnodes [8,10]. Pneumobilia on abdominal plain film suggests gallstone ileus and the diagnosis of enterolith ileus can be established only after documenting the normal gall bladder [10]. In our patient, pre-operative liver function test and CT scan did not revealed any biliary abnormality. This case thus serves as a reminder that gallstone like calculi can occur in a Meckel’s diverticulum.
To conclude, Meckel’s diverticulum should be considered in elderly patients with acute abdomen in whom cause of abdominal catastrophe is not clear, as complication of Meckel’s diverticulum including perforation could be fatal if not diagnosed early.
References
Fig. 3: Specimen showing perforated Meckel’s diverticulum with enterolith and appendix
Discussion
Enteroliths in association with Meckel's diverticulum have been rarely described in literature. Authors of one study reviewed the records of 776 patients with Meckel diverticulum and found stones in only two patients while a study conducted at Armed Forces Institute of Pathology reported a much higher incidence in which 8 of 84 cases in 24 years contained stones [5,6] .
The alkalinity of the distal small bowel favours precipitation of mineral salts which along with pooling of intestinal content and inspissation leads to enterolith formation [7]. Stone formation in Meckel's diverticula occurs more commonly in diverticula that do not usually contain ectopic gastric mucosa [8]. Enteroliths originating from a Meckel's diverticulum have also been associated with intestinal perforation [7,9].
Accurate diagnosis of diverticular perforation due to enterolith impaction is generally demanding. In abdominal X-ray, radio-opaque Meckel's enteroliths can be visualized in 20-25% of the cases suggesting that Meckel's enteroliths should be included in the differential diagnosis of abdominal calcification [4]. However, small bowel contrast studies and imaging modalities such as CT scan have been considered more useful. Ileus or perforation due to Meckel's enterolith must be differentiated from gallstone enterolith, appendicolith, teratoma and calcified lymphnodes [8,10]. Pneumobilia on abdominal plain film suggests gallstone ileus and the diagnosis of enterolith ileus can be established only after documenting the normal gall bladder [10]. In our patient, pre-operative liver function test and CT scan did not revealed any biliary abnormality. This case thus serves as a reminder that gallstone like calculi can occur in a Meckel’s diverticulum.
To conclude, Meckel’s diverticulum should be considered in elderly patients with acute abdomen in whom cause of abdominal catastrophe is not clear, as complication of Meckel’s diverticulum including perforation could be fatal if not diagnosed early.
References
- Pollak R. Adjunctive Procedure in Intestinal Surgery. In: Fischer JE (eds). Mastery of Surgery. Fifth edition. Philadelphia: Lippincott Williams & Wilkins; 2007, pp. 1392-1393.
- Stanley W. Ashley Edward E. Whang. Small Intestine. In: Brunicardi FC. Schwartz’s Principles of Surgery Eighth edition. USA: The McGraw Hill Companies; 2005.
- Yorganci K, Ozdemir A, Hamaloglu E, Sokmener C. Perforation of acute calculous Meckel's diverticulitis: A rare cause of acute abdomen in elderly. Acta Chir Belg. 2000;100(5):226-227.
- Umesh Gadhia, D. Raju, Rajeev Kapoor. Large enterolith in a meckels diverticulum causing perforation and bowel obstruction: An interesting case with review of literature. Indian J Surgery 2012, DOI:10.1007.
- Pantongrag-Brown L, Levine MS, Buetow PC, Buck JL, Elsayed AM. Meckel's enteroliths: clinical, radiologic, and pathologic findings. AJR Am J Roentgenol.1996;167:1447-1450.
- H. Wouter van Es, Sybrandy R. Enteroliths in a Meckel Diverticulum. Radiology 2000;214:524-526.
- Tosato F, Corsini F, Marano S, Palermo S, Piraino A, Carnevale L, et al. Ileal occlusion caused by enterolith migrated from Meckel's diverticulum. Ann Ital Chir. 2000;71:393-396.
- Kyriazanos ID, Tambaropoulos K, Martinos H, Pechlivanidis G, Davidis D, Noussis G. . Meckel's diverticulum lithiasis: A case of small bowel obstruction due to a migrated Meckel's Enterolith. Indian J of Surgery 2006;68 (1):41-43.
- Gibney EJ. Diverticulum of a Meckel's diverticulum containing a stone Postgrad Med J. 1991;67:692 - 694.
- Kusumoto H, Yoshida M, Takahashi I, Anai H, Maehara Y, Sugimachi K. Complications and diagnosis of Meckel's diverticulum in 776 patients. Am J Surg. 1992;164:382-383.
|