6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffbcf8010000000a01000001000d00
6go6ckt5b5idvals|157
6go6ckt5b5idcol1|ID
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Obstructed labor due to mechanical cause is a common entity but vesical calculi causing dystocia is extremely rare and very few cases have been reported in literature till date. If neglected, grave complications like vesico-vaginal fistula and uterine rupture can occur. Thus, timely diagnosis and early caesarean section should be done to prevent morbidity and mortality.
Case Report
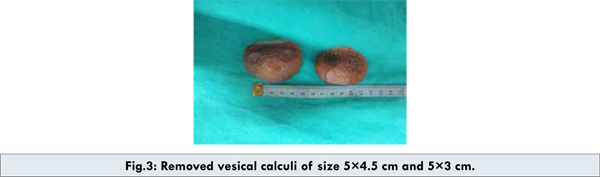
Mrs. X, 30 years old, primigravida was admitted with labour pains at 36 weeks of gestation. There was no present or past history of urinary complaints. Her general physical examination was normal. Abdominal examination revealed term size uterus, longitudinal lie, cephalic presentation, head 4/5th palpable above pelvic brim and regular fetal heart rate with good uterine contractions. Vaginal examination revealed bulging anterior vaginal wall due to the presence of two stony hard masses of sizes 5x5 cm and 5x4 cm, cervix was 2 cm dilated, 50% effaced, pushed to left side of pelvis due to the mass and vertex at -3 station. A provisional diagnosis of vesical calculi was made which was confirmed on ultrasonography. Ultrasonography showed two bladder calculi of sizes 5×4 and 5×3 cm [Figure 1]. Caesarean section was performed in view of mechanical dystocia. Simultaneous cystotomy [Figure 2] was performed and with the removal of two large calcium phosphate stones measuring 5×4.5 cm and 5×3 cm and weighing 66 and 46 grams respectively [Figure 3]. Her catheter was removed after 10 days and was discharged on 11th postoperative day.


Discussion
Dystocia due to vesical calculus is a rare condition. However, the absence of urinary symptoms in our patient with vesical calculi before and during pregnancy is rather unusual. Her condition remained undiagnosed as no antenatal ultrasound was performed. The common complications of vesical calculus during pregnancy are infection, abortion, premature deliveries and urinary fistula [1]. Very rarely uterine rupture has also been reported [2]. The diagnosis of dystocia by bladder stone is generally easy when the stone is large and palpable by vaginal examination as in our case [3]. The differential diagnosis of pelvic bone tumors, vaginal or bladder neoplasms and fibroids should be kept in mind. In some doubtful situations, the ultrasonography and radiography of the urinary tract may be useful, but they are always limited by the interposition of the fetal presentation.
Obstetrical management of an obstructed labor by a large bladder stone depend on the stage of labor and the possibility to push the stone out of the birth canal to allow the descent of the fetal head. When this maneuver is successfully performed the vaginal delivery can be possible, but if not, a cesarean section should be performed. Seth et al reported only three vaginal delivery out of ten pregnancies with vesical calculus [4]. Treatment of the vesical calculus depends on the mode of delivery. If a cesarean section is performed the calculus could be simultaneously removed, as in our case. However, the cystotomy during a cesarean section could increase the risk of urinary fistula. In the literature, two out of the six patients who had surgical removal of the calculus during the cesarean section, had developed vesico-cutaneous and a vesico-vaginal fistula [3,5]. However, in these two cases the cesarean section was performed after a prolonged labor, which may have caused pressure necrosis and urinary fistula. These complications can be prevented if diagnosis is made early in pregnancy and mode of delivery is decided accordingly.
Conclusion
Vesical calculi are rare cause of dystocia. The diagnosis is typically made by patient’s history, clinical examination and routine antenatal ultrasound. Mode of delivery can be planned according to the size and location of the stone. Complications can be prevented by timely diagnosis and proper management. When a cesarean section is indicated, intraoperative cystotomy with removal of the calculus is mandatory, even if it seems to increase the risk of urinary fistula.
Consent: Patient has given his or her informed consent for the case report to be published.
References
- Ait Benkaddour Y, Aboulfalah A, Abbassi H. Bladder stone: uncommon cause of mechanical dystocia. Arch Gynecol Obstet. 2006;274:323-324
- Kumar AG, Sharma S, Singh H, Singh S. Gravid Uterus - A Rare Case. Ind J Radiol Imag. 2004;14:433-434
- Penning SR, Cohen B, Tewari D, Curran M, Weber P. Pregnancy complicated by vesical calculus and vesicocutaneous fistula. Am J Obstet Gynecol. 1997;176:728–729.
- Seth S, Malik S, Salhan S. Vesical calculus causing dystocia. Eur J Obstet Gynecol Reprod Biol. 2002;101:199–200.
- Cope E. Obstructed labor due to vesical calculus. J Obstet Gynecol Br Commun. 1961;68:476.