6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffc49c02000000bc01000001000200
6go6ckt5b5idvals|185
6go6ckt5b5idcol1|ID
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Penile Mondor’s disease is a rare entity which occurs due to thrombosis of the superficial dorsal vein of the penis. The swelling involves the penile sulcus in a circumferential manner. Usually it is a self limiting condition with spontaneous resolution. The symptomatology includes penile swelling and pain. The diagnosis is usually missed and causes undue patient anxiety. Prompt diagnosis with reassurance goes a long way in the management of Penile Mondor’s disease.
Case Report
37 year old married male presented with the complaints of swelling in the penis associated with pain for the past 4 days [Fig.1]. The pain was sudden in onset, throbbing in nature, progressed rapidly with no response to antibiotics. There was no history of fever, coagulation disorder, urinary complaint, vigorous sexual activity or trauma preceding the complaints. He did not have any co-morbidity, history of smoking, prior surgery or sexually transmitted diseases. He was very concerned and anxious about the diagnosis and his future sexual function.

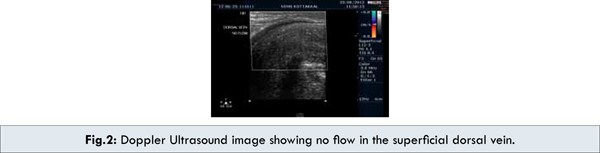
On examination, a thickened cord like tender swelling was palpated on the dorsal aspect of the penis. The cord like swelling extended from the pubic symphysis to the coronal sulcus. Circular edema was noted just proximal to the coronal sulcus. There were no enlarged inguinal lymph nodes. He was diagnosed clinically to have Penile Mondor’s Disease. All his laboratory tests and coagulation profile were normal. Doppler Ultrasound revealed thrombosis in the superficial dorsal vein with no flow and it was not compressible [Fig. 2]. He was reassured and the natural course of the disease was explained. He was managed with nonsteroidal anti-inflammatory agents and saline compresses. He was advised sexual abstinence for a month till the symptoms resolved.
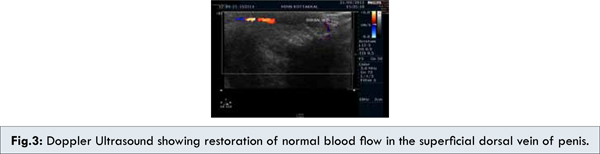
His 1 month follow up revealed resolution of symptoms, disappearance of swelling with normal sexual life. Doppler ultrasound revealed restoration of normal blood flow in the superficial dorsal vein [Fig. 3].
Discussion
French Surgeon Henry Mondor initially described thrombosis of the superficial vein of the anterolateral thoraco-abdominal wall in 1939. Thrombophlebitis of the superficial dorsal vein of the penis was first described by Braun-Falco in 1955 [1]. This condition was further highlighted by Helm and Hodge in 1958 [1]. The etiology is poorly understood and most cases are idiopathic. The predisposing factors suggested are trauma, vigorous sexual activity, surgery, malignancy, prolonged abstinence, contact with menstrual blood and long flight journey [2,3]. Usually they are seen in sexually active men. Sexual injury like stretching and buckling can lead to the endothelial injury and release of thrombotic substances which initiates the coagulation cascade [4]. Coagulation abnormalities like protein C, protein S and antithrombin deficiency have been considered as risk factors. These factors all depend on the Virchow’s triad–endothelial injury, stasis of blood and hypercoagulable state [3]. Association with sexually transmitted diseases were noted [5]. One case of association with sickle cell disease has also been reported [6].
The differential diagnosis includes Peyronie’s disease, sclerosing lymphangitis and fracture of the penis [7]. The diagnosis can usually be made on physical examination. Doppler ultrasound serves as an adjunctive tool – which shows noncompressible vein with no demonstrable flow within it [8]. The most important factor in the management of penile Mondor’s disease is reassurance which alleviates the patient’s anxiety. The role of antibiotics is not clear but it may be useful when cellulitis is present. Nonsteroidal anti-inflammatory agents serve the dual purpose of reducing the pain as well as acting against inflammation. Anticoagulation has also been tried but of no proven benefit. Penile Mondor’s disease is known for its spontaneous resolution and usually subsides within 3 to 6 weeks. If symptoms persist despite conservative treatment, excision of the thrombus may be indicated.
Conclusion
This case is highlighted due to the rarity of this condition and for the fact that the diagnosis is usually missed. An urologist should certainly be aware of this rare entity to avoid misdiagnosis and over treatment. The most important part in the management is proper diagnosis and reassurance of no sexual dysfunction to the patient.
References
- Kartsaklis P, Konstantinidis C, Thomas C, Tsimara M, Andreadakis S, Gekas A. Penile Mondor’s disease: a case report. Cases Journal. 2008;1:411. \
- Day S, Bingham JS. Mondor’s disease of the penis following a long-haul flight. Int J STD AIDS. 2005;16:510-511.
- Gigli F, Beltrami P, Arancio M, Zattoni F. Mondor’s penile disease: personal experience. Journal of Andrological Sciences. 2008;15:152-157.
- Kraus S, Lüdecke G, Weidner W. Mondor’s disease of the penis. Urol Int. 2000;64:99-100.
- Kumar B, Narang T, Radotra BD, Gupta S. Mondor’s disease of penis: a forgotten disease. Sex Transm Infect. 2005;81:480–482.
- Nachmann MM, Jaffe JS, Ginsberg PC, Horrow MM, Harkaway RC. Sickle cell episode manifesting as superficial thrombophlebitis of the penis. J Am Osteopath Assoc. 2003;103:102-104.
- Nazir SS, Khan M. Thrombosis of the dorsal vein of the penis (Mondor’s Disease): A case report and review of the literature. Indian J Urol. 2010;26:431-433.
- Machan K, Rojo-Carmona LE, Marquez-Moreno AJ, Herrera-Imbroda B, Ruiz-Escalante JF, Herrera-Gutierrez D et al. Ultrasound diagnosis of three cases of Mondor’s disease. Arch Esp Urol. 2012;65:262-266.