6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff2473300000007206000001000400
6go6ckt5b5idvals|2029
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Case Discussion
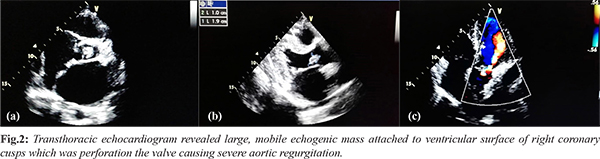
A 20-year-old male presented with intermittent, high grade fever of 2 weeks’ duration and palpitation with progressively worsening dyspnea. On examination, he had tachycardia, pulsus bisferiens and early diastolic decrescendo murmur along left sternal border suggestive of aortic regurgitation (AR). There were irregular, erythematous, flat, painless macules on tips of fingers and palms and plantar surfaces of toes and soles [Fig.1] for past one week which were diagnosed as Janeway lesions. Linear blackish-brown streaks were also noted on distal portions of great toes and nail plates of few fingers, which were diagnosed as splinter hemorrhages. Transrthoracic echocardiogram revealed large, mobile echogenic mass (10×19 mm) attached to ventricular surface of right coronary cusps which was perforating the valve causing severe leak [Fig.2]. Based on these findings, he was diagnosed to have acute severe AR with infective endocarditis having cutaneous stigmata of Janeway lesions and splinter haemorrhages. Broad spectrum antibiotics were started and he underwent successful aortic valve replacement after getting his informed consent.

Janeway lesions, initially believed to be small-vessel vasculitis, are result of minute septic emboli which stems from valvular vegetations leading to formation of dermal micro abscesses with thrombosis [
1]. Splinter haemorrhages are tiny blood clots that run vertically under the nails. They are non-specific cutaneous markers of endocarditis as have been reported in various connective tissue disorders, anti-phospholipid syndrome, hematological malignancy, and trauma [
2]. These cutaneous stigmata are seldom seen now as most of IE are diagnosed and treated early but still serve as important diagnostic clue to serious cardiovascular disturbance.
References
- Alpert JS. Osler’s nodes and Janeway lesions are not the result of small-vessel vasculitis. Am J Med. 2013;126:843-844.
- Tosti A, Iorizzo M, Piraccini BM, Starace M. The nail in systemic diseases. Dematol Clin. 2006;24:341-347.