6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff6492300000007605000001000700
6go6ckt5b5idvals|2031
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Malignancy of the tongue accounts for 22-39% of all oral cavity malignancies. Intestinal-type adenocarcinoma (ITAC) of tongue is a rare entity, accounting for 2% of all the tongue malignancies [
1]. Till now, eight cases of primary intestinal adenocarcinoma and three cases of metastatic intestinal adenocarcinoma of the tongue have been reported. Over the years, many hypothesis have been proposed to explain its origin, but exact etiology is still unclear. Here, we present a case of primary adenocarcinoma left lateral tongue with cervical secondaries in the neck.
Case Report
A 65 years old male, presented to the outpatient department, with complaints of a mass on the left lateral tongue since last 6 months. This mass increased progressively in size, more rapidly over the last 2 months. This was also associated with pain on swallowing and tongue movements. The patient had a history of chronic bidi smoking. There was no history of any other medical conditions or co-morbidities or any other significant family history.
On examination, an ulcero-proliferative mass was seen along left lateral tongue extending from 2 cm posterior to the tip upto the base of tongue [Fig.1]. On palpation the mass was firm, tender and bled on touch. On neck examination, a 2×2 cm lymph node was noted in the left level II and 1.5×1 cm lymph node in the level V. On palpation, they were firm, non-tender, fixed with normal overlying skin.
The CECT neck revealed a proliferative lesion in the left lateral tongue extending to left superior gingivo-buccal sulcus, left retro-molar trigone posteriorly with metastatic left cervical lymphadenopathy [Fig.2]. A biopsy from the lesion, under local anaesthesia, for histopathological examination showed mucin stained cells arranged in tubule-glandular pattern, suggestive of adenocarcinoma [Fig.3].
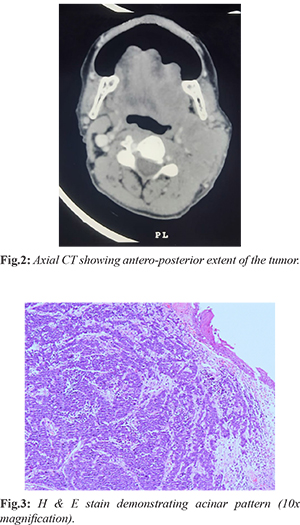
The specimen was further mounted and tested for certain markers by immune-histochemistry. The sample was positive for CK 7 and CK 20. Ki-67 was strongly positive. This was suggestive of intestinal-type adeno-carcinoma (ITAC). A fine needle aspiration cytology from the neck node showed malignant cells arranged in acinar pattern, suggestive of the possibility of adenocarcinoma. There were no lung metastases on chest X-ray. Ultrasound whole-abdomen, CT abdomen and panendoscopy ruled out presence of any intestinal malignancy. The patient was planned for chemo-radiotherapy. He was started on the first cycle of cisplatin and capecitabine. Owing to the advanced stage and rapidly proliferating nature of the disease, the patient expired during the course of treatment.
Discussion
ITAC of the tongue is an extremely rare disease entity. To date only 8 cases of primary ITAC of the tongue have been reported. A review of the eight reported cases of primary ITAC showed 3 cases arising from the base of the tongue [
2,
3]; 2 cases arising from anterior tongue [
4]; 2 cases from the dorsum of tongue [
1,
3] and 1 case of middle third involvement [
5]. Of these 8 reported cases, only one patient died of the disease and the rest 7 were alive, with no recurrence.
ITACs of the head and neck commonly involve sino-nasal tract with most frequent involvement of ethmoid sinus (40%), followed by nasal cavity (25%) and the maxillary antrum (20%) [
3]. However, in the oral cavity only 15 cases (10 primary and 5 metastatic) have been reported so far. These are classified into papillary (18%), colonic (40%), solid (20%), mucinous, and mixed (approximately 20%) [
3,
6]. Of these, 8 cases were reported to be arising from the tongue. A number of theories have been proposed in attempt to explain the pathogenesis of this malignancy. The most accepted hypothesis is malignant transformation of minor salivary glands [
2,
3]. Another theory, suggests activation of the dormant progenitor embryonic cells in the base of tongue to become malignant [
2,
4]. Malignant transformation of choristomatous tissue of GIT origin can also be a possible origin of this tumor [
1,
5,
7,
8]. A survey of CK7 and CK20 expression in epithelial neoplasms showed that all cases of colonic carcinoma were positive for CK20, while only 5% were positive for CK7. CK7 helps in distinguishing colonic adenocarcinoma from salivary gland origin adenocarcinoma [
1]. The present case was positive for CK20 and CK7.
Although rare there is always a possibility of intestinal metastasis to the oral cavity. Therefore, full body workup, including evaluation of gastrointestinal symptoms, CT scan abdomen, panendoscopy and if possible, PET scan should be done to rule out any other malignancy present. The present case was positive for CK20 and CK7. In addition, intestinal malignancy was ruled out after abdominal ultrasound and CT scan. These findings support the possibility of a primary tongue ITAC in the present case. Being a rare carcinoma, there are no standardized treatment guidelines for primary tongue ITAC. In the reported cases, combined chemo-radiotherapy of cisplatin/capecitabine or carboplatin/capecitabine followed by intensity-modulated radiotherapy (IMRT) have been used. In the present case, the patient was started on cisplatin 60 mg/m2 day 1 and capecitabine 625 mg/m2 BD on days 1-21 repeated every 3 weekly.
Due to limited available literature, the prognosis of this carcinoma is unclear. Of the eight reported cases of primary ITAC, seven showed favourable prognoses, with only one case of mortality. The case presented above, showed an aggressive tumor in advanced stage, and the patient died within six months of onset of symptoms.
Conclusion
Primary tongue ITAC is an extremely rare malignancy of the head and neck region. In the cases reported, there is predilection for base of the tongue which may be confused for metastatic disease. The diagnosis of primary tongue ITAC from any metastatic intestinal adenocarcinomacan should be established by thorough clinical, radiological and histopathological evaluation.
Contributors: AC: manuscript editing, and patient management; DS: manuscript editing, references and patient management; MM: manuscript writing and patient management; KA: critical inputs into the manuscript and histopathology. AC will act as a study guarantor. All authors approved the final version of this manuscript and are responsible for all aspects of the study.
Funding: None; Competing interests: None stated.
References
- Guo C, Jia MQ, Wang L, Jia J. Primary intestinal-type adenocarcinoma of the tongue. International Journal of Oral and Maxillofacial Surgery. 2018;47(12):1523-1526.
- Slova D, Mondolfi AP, Moisini I, Levi G, Urken M, Zevallos J, et al. Colonic-type adenocarcinoma of the base of the tongue: a case report of a rare neoplasm. Head and Neck Pathology. 2012;6(2):250-254.
- Bell D, Kupferman ME, Williams MD, Rashid A, El-Naggar AK. Primary colonic-type adenocarcinoma of the base of the tongue: a previously unreported phenotype. Human pathology. 2009;40(12):1798-1802.
- Smith SM, Old M, Iwenofu OH. Primary lingual colonic-type adenocarcinoma: a rare and emerging distinct entity. Head and Neck Pathology. 2017;11(2):234-239.
- Rahimi S, Akaev I, Repanos C, Brennan PA, Dubois JD. Primary intestinal-type adenocarcinoma of tongue: a case report with immunohistochemical and molecular profiles and review of the literature. Head and Neck Pathology. 2017;11(2):186-191.
- Berg J, Manosalva RE, Coughlin A, Su YB, Huang TS, Gentry J. Primary intestinal type adenocarcinoma of the oral tongue: Case report and review of histologic origin and oncologic management. Head & Neck. 2018;40(7):E68-E72.
- Yee KK, Li Y, Redding KM, Iwatsuki K, Margolskee RF, Jiang P. Lgr5-EGFP marks taste bud stem/progenitor cells in posterior tongue. Stem cells. 2013;31(5):992-1000.
- Gorlin RJ, Jirasek JE. Oral cysts containing gastric or intestinal mucosa: An unusual embryological accident or heterotopia. Archives of Otolaryngology. 1970;91(6):594-597.