|
Errarhay.S, Mamouni.N, Mahmoud.S, El fatemi.H1, Saadi.H, Mesbahi.O2, Squalli.N3, Bouchikhi.C, Amarti.A1, Banani.A
From the Department of Gynecology and Obstetrics; Department of Pathology1; Department of Oncology2; Department of Radiology3; University Hospital of Fez, Morocco.
Corresponding Author:
Dr. Errarhay Sanâa
Email: suine_err@yahoo.fr
Abstract
Introduction: Malignant melanoma, which has a highly malignant potential, is a tumor of the skin and mucosal membranes. Malignant melanomas of the female genital tract, including the vulva and vagina, are rare. Their overall prognosis is poor and is worse than that for cutaneous melanomas.
Cases presentation: Clinical data for 3 patients with primary malignant melanoma are presented. Diagnosis was based on histologic and immunohistochemical examinations. Case 1 was a 45 year-old women with cervical polyp and excision revealed malignant melanoma. Case 2 was 46-year-old woman with cervical and vaginal melanoma and the third was a 64 year-old women with lentiginous melanoma of the clitoris. One patient was treated with surgery and adjuvant chemotherapy, and two patients received systemic chemotherapy.
Conclusion: Although malignant melanoma of the female genital tract is uncommon, literature review shows that prognosis is poor than at other sites, most probably due to more advanced disease at diagnosis. This presentation highlights that early diagnosis by physicians at this relatively rare site is of crucial importance since it may result in improved outcome, similar to that of melanoma at more common sites.
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff642903000000dd01000001000900 6go6ckt5b5idvals|204 6go6ckt5b5idcol1|ID 6go6ckt5b5|2000F757Tab_Articles|Fulltext Case Series
Introduction
The foremost important etiological factor for malignant melanoma is considered to be sunlight exposure. However, primary lesions are also seen in non-sun-exposed areas. Elderly women should undergo regular gynecologic examinations and suspicious pigmented lesions should be biopsied. Herein, we attempt to increase physicians’ awareness for early diagnosis in order to improve prognosis.
Approximately 3% of malignant melanoma (MM) involves the female genital tract. The prognosis currently tends to be very poor, with a 5-year survival rates of 8.4%, regardless of treatment, which usually involves primary surgery (conservative or radical), and adjuvant radiotherapy or systemic chemotherapy regimens [ 1, 2]. The authors discuss three cases of gynecological melanoma and analyze clinical and prognostic aspects of this disease.
Case Reports
Case 1:
A 45-year-old woman was referred to our hospital with complaint of vaginal bleeding. Her medical history was unremarkable, and there was no family history of malignancy. Examination revealed a necrotic cervical lesion, 5 cm in size. A cervical papanicolaou test showed malignant infiltrative cells. Magnetic resonance imaging (MRI) revealed cervical lesion displacing the rectum to the back with signs of invasion [Fig.1]. Imaging studies revealed no evidence of metastases. An excision biopsy of the lesion suggested several possible diagnoses, including undifferentiated leiomyosarcoma or malignant melanoma. Immunohistochemistry showed HMB-54 and S-100 and CD117 positive staining, and the diagnosis was confirmed as malignant melanoma. Surgery was not indicated given the advanced stage of disease. The patient received chemotherapy; she had the third course with good development and good tolerance.
Case 2:
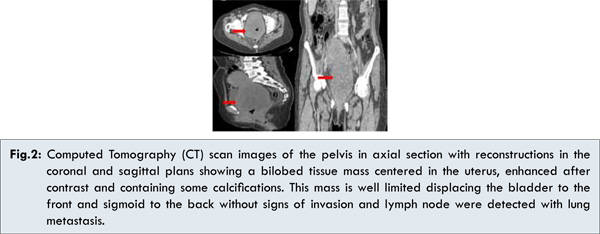
A 46 year-old woman presented with a complaint of vaginal bleeding. Her medical history was unremarkable, and there was no family history of malignancy. Examination revealed a cervical necrotic lesion, 10 cm in size, and another irregular lesion, 3 cm in size, on the anterior right side of the lower third of the vagina. Computed Tomography (CT) scan images of the pelvis in axial section with reconstructions in the coronal and sagittal plans showed a bilobed tissue mass centered in the uterus and enhanced after contrast and containing some calcifications, this mass displaced the bladder to the front and the sigmoid to the back without signs of invasion and lymph node were detected with lung metastasis [Fig.2]. A biopsy of the lesions was performed, and the histologic diagnosis was confirmed by positive immune-staining with monoclonal antibody to human melanoma (HMB-45), S-100 and CD-117. Surgery was not indicated given the advanced stage of disease. The patient received chemotherapy.
Case 3:
A 64-year-old woman, menopausal for 10 years, presented with a palpable mass in the vulva. Her medical history included hysterectomy and bilateral salpingo-oophorectomy. On vulvae examination, a lentiginous lesion, 3×2 cm in size, was seen in the clitoris and bilateral inguinal lymph nodes were palpable [Fig.3]. Following vulvar biopsy, mucosal lentiginous malignant melanoma was diagnosed and the histologic diagnosis was confirmed by positive immune-staining with monoclonal antibody to human melanoma (HMB-45), S-100 and CD-117 [Fig.4,5]. Thoraco-abdomino-pelvic computed tomography (CT) revealed lung metastasis and lymph node. She was treated with wide local excision of the tumor (excision of 2 cm from the outer limit and 2 cm from the deep limit of the tumor) and bilateral inguinal lymph node dissection. No tumor tissue was present in the surgical margins, and lymphatic invasion was found. The patient received chemotherapy with good tolerance.
Discussion
Malignant melanomas are generally found in areas of skin exposed to the sun, but can also be present in non exposed sites, such as genital tract. The first case of malignant melanoma of the female genital tract was reported by Hewitt in 1861 [ 3].
Differential diagnosis between a primary cervical melanoma and a metastatic tumor is important because the latter can be part of a metastatic disease spreading to the cervix. At the present moment, there is no standard treatment for this disease, while there is no doubt that the surgical approach is the most usual and radical hysterectomy with or without pelvic lymphadenectomy and/or superior vaginectomy is reported most frequently [ 4- 7], some authors entertain doubts concerning survival if pelvic lymphadectomy is performed [ 6]. Although there is no enough information about the real role of negative margins in primary melanoma of the cervix, the primary surgery should have the purpose of obtaining negative margins [ 8]; some authors recommend minimum margins of 2 cm [ 7]. The role of radiotherapy has not been well established, but it has been demonstrated that radiotherapy reduces the tumor size [ 4, 5]. The use of adjuvant pelvic radiotherapy is considered in the case of not obtaining satisfactory surgical resection margins, parametrium involvement, or when lymph nodes are found to be involved [ 8].
Despite the low level of radiosensitivity exhibited by melanoma, the use of external or intracavitary radiotherapy is recommended after surgery, or palliatively when the tumor is inoperable. In the current study, chemotherapy was chosen in case 1 and surgery was not indicated given the advanced stage of disease [ 4, 5, 8]. In gynecological melanoma, no chemotherapy regimens have been reported that substantially may reduce the possibility of recurrence. Dacarbazine is utilized in advanced disease, as the case for our patients, and it has been observed that up to 20% of patients may have response [ 7, 8].
Primary vulva melanoma is the second most common malignancy arising within the vulva and accounts for 8-10% of all vulvar malignancies. Parity, hormonal and genetic factors seem to be unrelated to the occurrence of vulvar melanoma [ 9]. Common presenting symptoms include a palpable vulvar mass, pain, bleeding and itching. Our patient with vulvar melanoma presented with a lentiginous lesion. An increased awareness of pigmented vulvar lesions and a low clinical threshold for biopsy of such lesions may ultimately hold the best hope for improving the prognosis in susceptible patients.
The main prognostic factors are demographic characteristics, tumor localization, presence of groin node metastases, and various tumor characteristic. Age, stage and lymph node involvement were found to be significant factors affecting survival in patients with vulvar melanoma [ 10].
In 1997, Luxman et al [ 11] presented a case of uterine metastasis from vulvar malignant melanoma. Recently, Akoz et al [ 12] reported a synchronous cervical and vulvar malign melanoma. These studies demonstrate the importance of evaluating the entire genital system in patients with vulvar melanoma.
The recommended treatment for vulvar melanoma has been radical vulvectomy with bilateral inguino-femoral lymphadenectomy, regardless of lesion size, thickness, or depth of invasion [ 13, 14]. However, most authors conclude that radical surgery does not improve the survival of patients with early disease when compared to local excision. However, such radical surgery, which is disfiguring and associated with severe morbidity, has not been shown to improve the survival of patients with vulvar malignant melanoma and, thus, has been questioned. But a small safety distance could be accompanied with a high risk of local progression.
The recommendations for treatment of vulva melanomas with thin lesions (<1 mm) are wide local excision with a safety distance of 1 cm and, with deeper lesions, an en bloc resection with safety distance of 2-3 cm with regional (inguino-femoral) lymphadenectomy [ 15]. In intraoperative examinations, the pathologist cannot safely distinguish invasive melanoma from melanoma in situ. Thus, it is advisable that maculous lentiginous hyperpigmentated areas should be excised.
Although the duration of follow-up was shorter in those patients who underwent less radical surgery, the absence of recurrence in patients with lesions of a depth of 2 mm or less suggests that patients with superficial lesions may be spared the morbidity of radical resection. Patients with vulvar melanoma lesions deeper than 4 mm have a high risk of distant metastases that is unlikely to be significantly decreased, even with the use of radical vulvectomy and bilateral inguinofemoral lymphadenectomy.
Vulvar melanomas have an overall poor prognosis, and there is a lack of consensus in the published literature regarding treatment options. Surgery is still the best available treatment for the control and potential cure of malignant melanomas. However, the therapy should be tailored to meet the specific needs of individual patients [ 16]. Dacarbazine is the most active chemotherapeutic agent, which can produce response rates of 15-25% [9]. The third case was treated with wide local excision of the tumor (excision of 2 cm from the outer limit and 2 cm from the deep limit of the tumor) and bilateral inguinal lymph node dissection. No tumor tissue was present in the surgical margins, and lymphatic invasion was found and she received chemotherapy with good tolerance.
Primary malignant melanoma of the vagina is a rare tumor, with fewer than 300 cases reported worldwide. It accounts for less than 3% of all vaginal malignancies and for 0.3-0.8% of all malignant melanomas [ 17]. As the vagina has a diffuse lymphatic plexus and the tumor can spread hematogenously, early metastases are common. Clinical diagnosis is often made at an advanced stage with a variable degree of pigmentation, usually on the anterior aspect of the vagina. However, lung metastasis was detected in our patient with vaginal melanomas at the time of diagnosis. The most common presenting symptoms are vaginal bleeding, vaginal discharge or a palpable mass. The tumors are most commonly located in the distal third of the vagina and mostly on the anterior wall, as in our patient.
Several treatment options exist, but no standard approach has been established. The spectrum of surgical therapies ranges from conservative surgery, such as wide local excision or total vaginectomy, to radical extirpation with en bloc removal of involved pelvic organs. Previous studies have recommended wide local excision with adjuvant radiotherapy, and radical surgery with adjuvant radiotherapy as second-line therapy. Both procedures result in similar 5-year survival rates. Some authors have recommended radical surgery, but more recent publications have reported that wide local excision is associated with equivalent survival rates. The role of elective lymph node dissection also remains controversial, as does the dissection of lymph nodes that are clinically negative for melanoma of the vagina.
Coleman et al [ 18] reported that routine lymphatic dissection is impractical, given the rich anastomotic nature of the vaginal lymphatics and the imperfect prediction of limited negative sampling. Miner et al [ 19] also suggested that elective pelvic lymph node dissection was not essential because of the low rate of lymph node metastasis. Sentinel lymph node mapping has recently gained popularity. Siu et al [ 20] recommended excluding lymphatic and distant metastases before embarking on radical surgery. Surgery was not indicated in case 2 given the advanced stage of disease. The patient received chemotherapy
Conclusion
The prognosis for malignant melanoma of the female genital tract is poor, regardless of the treatment delivered, though it can be improved if the disease is diagnosed early. As there is currently no proven standard therapy, therapy should be tailored to meet the specific needs of individual patients.
References
- Irvin Jr WP, Brliss SA, Rice LW, Taylor Jr PT, Andersen WA. Malignant melanoma of the vagina and loco-regional control: Radical surgery revisited. Gynocologic Oncology. 1998;71:476-480.
- Bonner JA, Perez-Tamayo C, Reid GC, Roberts JA, Morley GW. The management of vaginal melanoma. Cancer. 1988;62:2066-2072.
- Hewitt P. Sequel to a case of recurrent melanosis of both groins and back: The disease reappearing in the brain, heart, pancreas, liver and other organ. Lancet Oncology. 2008;9:973-981.
- Siozos C, Bhat A, Lonsdale R, Nieto JJ, Crocker SG. Malignant melanoma of the uterine cervix. Journal of Obstetrics and Gynecology. 2005;25:826-827.
- Baruah J, Roy KK, Kumar S, Kumar LA. Rare case of primary malignant melanoma of cervix. Archives of gynecology and Obstetrics. 2009;280:453-456.
- Wasef WR, Roberts JK, Dixon GR. Primary malignant melanoma of the cervix uteri. Journal of Obstetrics and Gynecology. 1999;19:673-674.
- Canturia G, Angioli R, Nahmias J, Estape R, Penalver M. Primary malignant melanoma of the uterine cervix. Gynecol Oncol. 1999;75:170-174.
- Piura B. Management of primary melanoma of the female urogenital tract. The Lancet Oncology. 2008;9:973-981.
- Irvin WP Jr, Legallo RL, Stoler MH, Rice LW, Taylor PT Jr, Andersen WA. Vulvar melanoma: a retrospective analysis and literature review. Gynecol Oncol. 2001;83:457-465.
- Sugiyama VE, Chan JK, Shin JY, Berek JS, Osann K, Kapp DS. Vulvar melanoma: a multivariable analysis of 644 patients. Obstet Gynecol. 2007;110:296-301.
- Luxman D, Jossiphov J, Cohen JR, Wolf Y, David MP. Uterine metastasis from vulvar malignant melanoma. A case report. J Reprod Med. 1997; 42:244-246.
- Akos I, Ayas S, Eren S, Bilgic R. Synchronous cervical and vulvar malign melanomas: metastasis or multifocality of the disease? A case report and review of the literature. Int J Gynecol Cancer. 2006;16:917-920.
- Reid GC, Schmidt RW, Roberts JA, Hopkins MP, Barrett RJ, Morley GW. Primary melanoma of the vagina: A clinic-pathologic analysis. Obstet Gynecol. 1989;74:190-199.
- Stellato G, Lodice F, Casella G, Fortuna G, Tramontana R, di Bonito M, Tramontana S. Primary malignant melanoma of the vagina: case report. Eur J Gynecol Oncol. 1998;19:186-188.
- Nakagawa S, Koga K, Kugu K, Tsutsumi O, Taketani Y. The evaluation of the sentinel node successfully conducted in a case of malignant melanoma of the vagina. Gynecol Oncol. 2002;86:387-389.
- Suwandinata FS, Bohle RM, Omwandho CA, Tinneberg HR, Gruessner SE. Management of vulvar melanoma andreview of the literature. Eur J Gynecol Oncol. 2007;28:220-224.
- Moros ML, Ferrer FP, Mitchell MJ, Romeo JA, Lacruz RL. Primary malignant melanoma of the vagina: poor response to radical surgery and adjuvant therapy. Eur J Obstet Gynecol Reprod Biol. 2004;113:248-250.
- Coleman RL. Primary vaginal melanoma: a rare and problematic clinical entity. Ann Surg Oncol. 2004;11:4-6.
- Miner TJ, Delgado R, Zeisler J, Busam K, Alektiar K, Barakat R, Poynor E. Primary melanoma: a critical analysis of therapy. Ann Surg Oncol 2004;11:34-39.
- Siu SS, Lo KW, Chan AB, Yu MY, Cheung TH. Nodal detection in malignant melanoma of the vagina using laparoscopic ultrasonography. Gynecol Oncol. 2004;92:985-988.
|