6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffc49603000000f601000001001500
6go6ckt5b5idvals|221
6go6ckt5b5idcol1|ID
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Gastric volvulus is rotation of all or part of stomach more than 180 degree causing close loop obstruction [
1]. This rotation can be organoaxial (along the long axis of stomach) or mesentricoaxial (perpendicular to long axis of stomach). Patient usually presents with Borchardt’s triad of epigastric pain and distention, retching or nonproductive recurrent vomiting and difficulty in nasogastric tube insertion and very rarely with signs of peritonitis in view of strangulation leading to perforation of stomach [
2-
4]. We are reporting a case of 14 year young girl who presented with strangulated gastric volvulus secondary to eventration of diaphragm. She was managed with partial gastrectomy and anterior gastropexy and plication of diaphragm with uneventful postoperative period.
Case Report
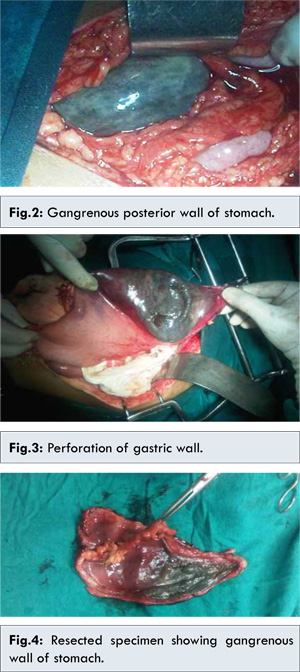
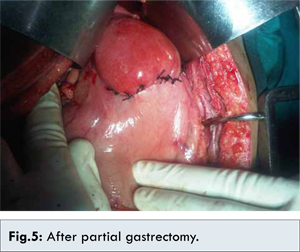
A 14 year old girl presented with history of upper abdominal pain and recurrent non bilious vomiting since last 2 days. Pain has increased in its intensity and diffused to whole abdomen since 6 hours. Past history of similar two episodes, managed conservatively by healthcare provider was present.There was no previous history of peptic ulcer disease, hematemesis and gastro esophageal reflux disease, jaundice, or any other systemic complaints. On examination she was drowsy and dehydrated with pulse 110/minute, blood pressure 96/60 mm Hg, respiratory rate of 18 per minute. Abdominal examination revealed tenderness, guarding, rigidity and sluggish bowel sounds. X-ray chest and abdomen revealed “gas” under right dome of diaphragm and eventration of left dome [Fig.1]. Laboratory investigations revealed-hemoglobin: 11 gm%, total leucocyte count: 11000/mm3, serum urea: 60 IU/dL (Normal 2-20 IU/dL), other investigations were within normal limits. Patient was resuscitated with crystalloids. Attempts to insert Ryle’s tube for nasogastric decompression were unsuccessful. Exploratory laparotomy revealed gangrenous posterior wall of stomach [Fig.2] due to volvulus and perforation in posterior wall of stomach [Fig.3]. There was associated eventration of diaphragm. Partial gastrectomy (resection of gangrenous part of stomach) [Fig.4,5] with anterior gastropexy and placation of diaphragm with prolene 2-0 was done. Postoperative period was uneventful. Patient was allowed orally on day 3 and discharged on day 6 of surgery.

Discussion
Gastric volvulus is a rare but potentially life-threatening entity [
5]. Incidence of gastric volvulus is not known since many cases remain undiagnosed by the treating physicians. Gastric volvulus has been classified into organoaxial: stomach rotates along longitudinal axis, associated with paraesophageal hernia and mesenteroaxial type: stomach rotates between the lesser and greater curvatures, idiopathic causing chronic features [
3,
6]. Anatomically it is classified as intrathoracic and intra-abdominal while on the basis of etiology: primary or secondary depending on presence of risk factors like hiatal hernia, diaphragmatic hernia or eventration or abdominal bands [
1,
5,
6]. This case of strangulated gastric volvulus occurred secondary to eventration of diaphragm.
Gastric volvulus can occur at any age, however, it is more common in children [
7]. The classic triad described by Borchardt’s of retching, severe and constant epigastric pain, and difficulty in inserting a nasogastric tube suggests an acute gastric volvulus [
2,
3]. This 14 year old girl presented with upper abdominal pain and recurrent non bilious vomiting and insertion of Ryle’s tube was unsuccessful. Traditionally acute gastric volvulus is diagnosed on chest X ray showing retrocardic air bubble or large air fluid level in the chest [
8]. X-ray chest and abdomen in our case revealed “gas” under right dome of diaphragm and eventration of left dome. A CT scan can lead to immediate diagnosis with anatomical details and should be the investigation of choice as it avoids any delay in diagnosis [
9]. But in acute emergency situations like this where CT scan was not possible, clinical and X ray finding remains only investigation. In emergency situations like this clinician should have high index of suspicion of gastric volvulus in patients presenting with Borchardt’s triad.
Treatment of choice in acute gastric volvulus is laparotomy with detorsion, anterior gastropexy. In cases of gastric strangulation the necrotic portion of stomach is resected [
1,
10]. Recurrent volvulus is prevented by anterior gastropexy and repair of diaphragmatic repair should be undertaken as was done in our patient.
Conclusion
Gastric volvulus is an uncommon cause of upper abdominal pain and persistent vomiting. This diagnosis must be suspected in patients with documented paraesophageal hernia and diaphragmatic eventration. The presence of persistent vomiting despite initial antiemetic treatment, continuing epigastric pain and inability to pass a nasogastric tube should trigger one to think of gastric volvulus. Early diagnosis and treatment can decrease the morbidity and mortality.
References
- S Singham, B Sounness. Mesenteroaxial volvulus in an adult: time is of the essence in acute presentation. Biomed Imaging Interv J. 2009; 5(3):e18.
- Chau B, Dufel S. Gastric volvulus. Emerg Med J. 2007;24:446-447.
- Borchardt M. ZurPathologie und Therapie des Magenvolvulus. Arch KlinChir. 1904;74:243–260.
- NurettinÖzgür DOGAN, Gökhan AKSEL, Ahmet DEMIRCAN, Ayfer KELES, Fikret BILDIK. Gastric volvulus due to diaphragmatic eventration and paraesophageal hernia. Turk J Med Sci. 2010;40:825-828.
- Shah NN, Mohsin M, Khursheed SQ, Farooq SS, Buchh AA, Quraishi AQ. Eventration of diaphragm with gastric volvulus: acase report. Cases J. 2008;1:404.
- Moy RK, Salazar AM, Chan SB. Inability to pass a nasogastric tube: a surgical emergency. Am J Emerg Med. 2007;25:213-215.
- Darani A, Mendoza-Sagaon M, Reinberg O. Gastric volvulus in children. J Pediatr Surg. 2005; 40:855-858.
- Andiran F, Tanyel FC, Balkanci F, Hiçsönmez A. Acute abdomen due to gastric volvulus: Diagnostic value of a single plain radiograph. PediatrRadiol. 1995;25Suppl. 1:S240.
- Coulier B, Ramboux A. Acute obstructive gastric volvulus diagnosed by helical CT. JBR-BTR. 2002;85:43.
- Flanagan NM, McAloon J. Gastric volvulus complicating cerebral palsy with kyphoscoliosis. Ulster Med J. 2003;72:118-120.