6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff7444050000006302000001000d00
6go6ckt5b5idvals|288
6go6ckt5b5|2000F757Tab_Articles|Fulltext
Introduction
Benign tumors of the endobronchial tree are rare, and among them lipoma is the least common with a documented evidence of 0.1-0.5% [
1-
3]. Although histologically benign in character these tumors are significant as they may simulate malignant tumors clinically. Also due to their endobronchial location, they can cause irreparable obstructive lung damage. We discuss one such case of endobronchial lipoma in the left lower lobe bronchus in a 45 year old woman.
Case Report
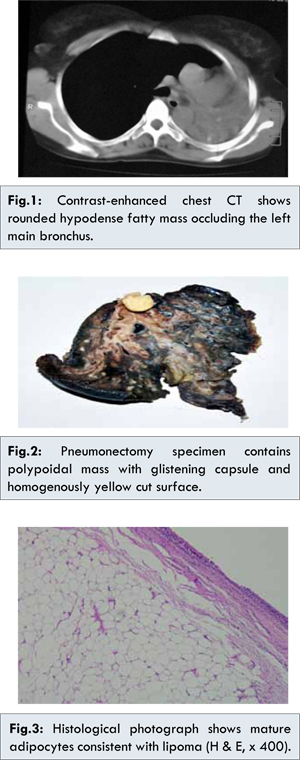
A 45 year old female was referred to LRS institute with complaints of cough with expectoration along with on and off fever for last 2 years. She also complained of chest pain for last 5 months. General physical examination revealed mild anemia. Other hematological and biochemical parameters were normal. Pulmonary function test showed moderate impairment of lung function. Chest X ray showed collapsed consolidated left lung. On bronchoscopy a polypoidal fleshy mass occluding the left main bronchus, about 2.5 cm away from the carina was found. Trachea, carina and bilateral vocal cords were normal. Computed tomography scan of the chest revealed a hypodense mass [Fig.1] in left main bronchus occluding it completely. There was collapse of the left main bronchus with extensive bronchiectatic changes.
A left pnemonectomy was performed. Histopathology specimen measured 11.5x9.5x5.5 cm and showed a broad based globular mass of size 1.5x1.2x1.2 cm protruding from left main bronchus [Fig.2]. The mass was attached to surface mucosa and appeared soft with glistening yellow surface. Cut section was also yellow in color. Lung parenchyma showed dilated bronchovascular channels with circumscribed creamish white areas measuring 0.3 to 0.6 cm in diameter. Microscopically, the tumor mass was composed of mature adipocyte which were univacoular and uniform in size [Fig.3]. The mass was covered by thin fibrous capsule and partly lined by respiratory epithelium. Lung parenchyma (due to chronic obstruction) showed changes of bronchiectasis, areas of chronic inflammation rich in lympho-plasmacytic cell and feature of organizing pneumonia. Tissue Ziehl Neelsen stain was negative. No other heterologous elements like fibrous, epithelial and glandular tissue along with cartilage and muscle was found. A diagnosis of endobronchial lipoma with changes of chronic bronchiectasis was rendered.
Discussion
Most tumors of the tracheobronchial tree are malignant (either primary bronchial carcinomas or metastatic lesions). Only 5% of them are benign, of which ninety percent are adenomas (mucous cell adenoma, pleomorphic adenoma and oncocytoma) or hamartoma [
3]. Lipomas constitute 3.2-9.5% of all benign endobronchial tumors [
3]. They have an incidence of 0.1-0.5% indicating that they are extremely rare [
1,
2]. They can also be found as intrapulmonary and mediastinal mass. Most of them arise from the fat cells in the submucosal layer of the main or lobular bronchus. Rarely, they arise from connective tissue between or outside the cartilage. Occasionally additional cell types, such as those of fibrous tissue, glandular tissue and cartilage may also be present.
Patients with tracheobronchial lipomas are generally in late middle age and with a definitive male preponderance. Unlike malignant tumors, endobronchial lipomas including other benign neoplasm of tracheobronchial tree present with symptom of obstruction including productive cough, hemoptysis and wheezing, recurrent pneumonia, bronchiectasis [
4,
5]. Depending upon the extent of obstruction, varying degree of irreversible lung damage can be found.
They may be misdiagnosed clinically, as a bronchial carcinoid or metastatic tumor, as their symptoms and complication are alike. Other conditions that are clinically indistinguishable include inflammatory psuedopolyp, broncholith and fungal infection. In this scenario, identification of the lesion either by endoscopic or radiological means may help avoids unnecessary delay in proper management and thus serious complications of the lung. The chest radiographic features of lipoma are nonspecific and typically related to obstruction like atelectasis, pneumonia, bronchiectasis and medistinal shift [
4,
5,
6]. Bronchoscopy also often does not provide a definite diagnosis due to the fibrous capsule of the lesion. However, CT is highly specific and sensitive in the detection of adipose tissue and CT finding of a pedunculated homogenous lesion with attenuation of around 100 HU can lead to definitive diagnosis of endobronchial lipoma [
3,
7]. However, endobronchial hamartomas which can contain fat besides cartilage, fibrous and epithelial tissue, also appear as a fatty mass on CT [
5,
6]. Therefore, whenever a fatty endobronchial mass is identified on CT, the differential diagnosis should include lipoma and hamartoma. In our case, patient presented with productive cough. CT scan showed endobronchial hypodense fatty mass occluding the left main bronchus completely, suggesting lipoma and hamartoma. Laser resection by bronchoscopy is considered the first choice of treatment in both lesions [
8]. However, in the case of delayed diagnosis and destruction of underlying lung lobectomy or pnemonectomy is often required as happened in the present case [
8].
Conclusion
Endobrochial lipoma is a rare benign neoplasm that may cause irreversible pulmonary damage distally and may be misdiagnosed clinically as a bronchial carcinoid or a malignant tumor. The accuracy of transbronchial biopsy is low but demonstration of homogenous fat attenuation by CT imaging can guide the differential diagnosis. Therefore, proper identification of the lesion by endoscopic and radiological means is required to avoid unnecessary complications and radical surgery of the lung.
References
- Jensen MS, Peterson AH. Bronchial lipoma. Scand J Thorac Cardiovasc Surg. 1970;4:131-134.
- Schraufnagel DE, Morin JE, Wang NS. Endobronchial lipoma. Chest. 1979;75:97-99.
- Pollefliet C, Peters K, Janssens A, Luijks A, Bouwel EV, Marck EV, et al. Endobronchial lipomas. Rare Benign Lung tumors, Two Case Reports. J Thorac Oncol. 2009;4:658-660.
- Ko JM, Jung JI, Park SH, Chung MH, Ahn MI, Kim KJ, et al. Benign tumors of the tracheobronchial tree: CT-Pathological correlation. Am J Roentgenol. 2006;186:1304-1313.
- Wilson RW, Kirejezyk W. Pathological and radiological correlation of endobrochial neoplasm. Part I. Benign tumors. Ann Diagn Pathol. 1997;1:31-46.
- Ahn JM, Im JG, Seo JW, Han HS, Yoon HK, Kim WS, et al. Endobronchial Hamartoma: CT findings in three patients. Am J Roentgenol. 1994;163:49-50.
- Gaerte SC, Meyer CA, Winer-Muram HT, Tarver RD, Conces DJ Jr. Fat containing lesions of the chest. Radiographics. 2002;22:S61-S78.
- Muraoka M, Oka T, Akamini S, Nagayasu T , Iseki M, Suyama N, et al. Endobronchial lipoma. Review of 64 cases reported in Japan. Chest. 2003;123:293-296.