6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffa4fe380000007106000001001000
Introduction
Paraganglioma like dermal melanocytic tumor (PDMT) is a recently described subtype of primary dermal melanocytic tumor [1]. It is considered as a unique benign neoplasm derived from melanocytes. Histologically the tumor cells are seen as nests of round or oval cells with amphophilic cytoplasm separated by thin fibrous strands [2]. PDMT is primarily a tumor seen in the extremities of adult females and presents as a non-pigmented dermal nodule averaging 1.4 cm in diameter. The lesion may be confused with other benign dermal tumors like cellular blue nevus and granular cell tumor or malignant dermal tumor like melanoma. PDMT is a very rare lesion with only thirteen cases reported so far.
Case Report
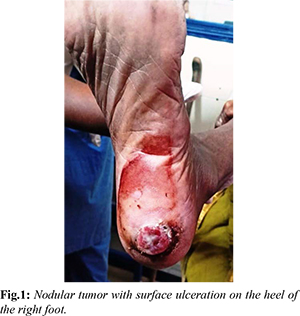
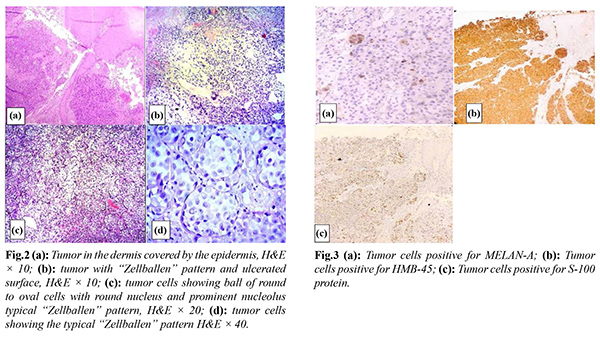
An 85-year-old woman presented to the surgical outpatient department with the complaint of an ulcerated nodular swelling on the heel of left leg. Two years ago, it began as a small nodule and has since grown to its current size. Recently, surface ulceration with bleeding has started [Fig.1]. Clinical examination didn’t reveal any other significant findings. X-ray revealed uninvolved bone underneath. Possibility of squamous cell carcinoma or a tropic ulcer was considered. An incisional biopsy was performed, and the tissue was sent for histopathological examination. The tissue that was received measured 1×1 cm, had an irregular, firm, grayish-white appearance, and was partially covered with skin. The cut surface of the tissue appeared grayish-brown. Microscopically, the examination revealed a nodular tumor in the dermis with an area of ulcerated surface [Fig.2]. The tumor in the dermis consisted of nests of oval or round tumor cells with one or two round nuclei and amphophilic cytoplasm. These nests were separated by thin fibrous septae [Fig.3]. There was no atypia or any increased mitotic activity. Immunohistochemical (IHC) stains of S-100 protein, MELAN-A and HMB-45 stains were positive and pancytokeratin stains were negative [Fig.4]. A diagnosis of paraganglioma like dermal melanocytic tumor (PDMT) was made basing on the positive IHC stains. The patient has undergone total excision of the lesion and she is doing well after 4 months of follow up.
Discussion
Deyrop et al. [1] coined the term PDMT, which is regarded as a subtype of benign dermal melanocytic tumor. PDMT mainly affects adult females between 18 to 53 years of age, presenting as single or multiple nodules on the extremities. As of now, there have been no reports of recurrence or metastasis from this lesion [3]. Only thirteen cases of this rare lesion have been reported in the world literature [Table 1] [1-6]. Interestingly, 8 out of the 10 cases reported by Deyrop et al. were diagnosed retrospectively while reviewing all dermal melanocytic tumors [4].
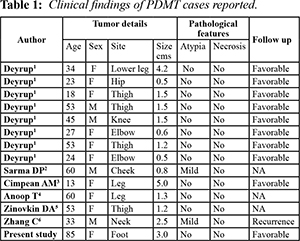
PDMT needs to be distinguished from other dermal tumors as cellular blue nevus, which is characterized by a poorly circumscribed, infiltrative proliferation, epidermal invasion, and lack of paraganglioma-like growth pattern. Other malignant tumors, such as primary/metastatic melanoma and clear cell sarcoma can be easily excluded because of high-grade nuclear features, high mitotic activity, infiltrative proliferation, and epidermal invasion [3]. PDMT can be distinguished from other lesions based on its histological features, which include the "Zellballen" pattern of tumor cells, the absence of atypia or hyperplasia of melanocytes, the lack of overlying epidermal hyperplasia, and the expression of S-100, HMB-45, and MELAN-A markers by tumor cells, while not expressing pancytokeratin markers [7]. The histological features observed in Hematoxylin and Eosin (H&E) stain strongly suggest "paraganglioma." Cutaneous paraganglioma is an extremely rare tumor, likely due to the absence of ganglia in cutaneous tissue. Additionally, paraganglioma cells do not express melanocyte markers. Therefore, considering the location of the lesion and strong positivity of the IHC stain, it is highly suggestive of a melanocyte origin.
PDMT is considered a benign process because of bland nuclear features, low mitotic activity, and no necrosis, although low malignant potential cannot be excluded [8]. Melanoma and dermal melanocytic tumor of uncertain malignant potential are excluded in our lesion based on the absence of nuclear atypia, mitoses and necrosis in the tumor.
Conclusion
PDMT is a rare type of dermal melanocytic tumor that can be easily mistaken for other melanocytic lesions or paraganglioma. Due to the limited availability of follow-up information and scarce reference materials, close monitoring is necessary for this seemingly benign tumor.
Contributors: HSN: acquisition and interpretation of the data; CB: analysis and revision of the data; DPGJ: clinical input and revision of the data. HSN will act as a study guarantor. All authors approved the final version of this manuscript and are responsible for all aspects of this study.
Funding: None; Competing interests: None stated.
References
- Deyrup AT, Althof P, Zhou M, Morgan M, Solomon AR, Bridge JA, et al. Paraganglioma like dermal melanocytic tumor: A unique entity distinct from cellular blue nevus, clear cell sarcoma and cutaneous melanoma. Am J Surg Pathol. 2004;28:1579-1586.
- Sarma DP, Bryan T, Bo W. Paraganglioma like dermal melanocytic tumor: A case report. Cases J. 2008;1:48.
- Cimpean AM, Ceausu R, Raica M. Paraganglioma- like dermal melanocytic tumor: A case report with particular features. Int J Clin Exp Pathol. 2010;3:222-225.
- Anoop T, Bindurani S, Geetha K, Rajiv S, Robins K. Paraganglioma-like dermal melanocytic tumor. Indian J Dermatol. 2015;60:80-81.
- Zinovkin DA, Aliakskinski VS, Hryb AK, Dedik SYu. Paraganglioma-like dermal melanocytic tumor: A rare skin lesion. Exp Oncol. 2015;37:156-157.
- Zhang C, Chen C, Hu H, Yan X. Primary paraganglioma-like dermal melanocytic tumor with local recurrence: a case report. Int J Clin Exp Pathol. 2018;11:2875-2878.
- Weedon D. Lentigenes. Nevi and melanomas. In: Weedon D, editor. Weedon’s Skin Pathology. 2nd ed, China: Elsevier Publishing; 2016; p. 863.
- Elder DE, Murphy GF. Atlas of tumor pathology: melanocytic tumors of the skin. Washington, DC: Armed Forces Institute of Pathology; 2010: p.183-185.