Introduction
Hemothorax, the accumulation of blood in the pleural cavity, is a common complication of thoracic trauma and is often associated with rib fractures [1,2]. However, it may also occur in the absence of obvious initial radiological findings. While most cases present immediately after injury, delayed hemothorax can develop hours to days later despite a normal initial chest X-ray, making diagnosis challenging.
This highlights the importance of maintaining a high index of suspicion, ensuring proper follow-up, and considering repeat or advanced imaging in patients with persistent or worsening symptoms after blunt chest trauma.
Case Report
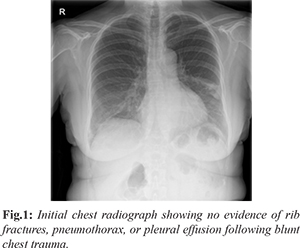
We report the case of a 64-year-old woman who sustained a fall, resulting in blunt trauma to the right side of the chest. She was initially evaluated at the Urgent Care Service, where clinical examination was unremarkable. Chest radiography demonstrated no evidence of rib fractures, pneumothorax, or pleural effusion [Fig.1]. The patient was discharged with analgesics and provided with safety-netting advice, including instructions to seek medical attention if her symptoms worsened.
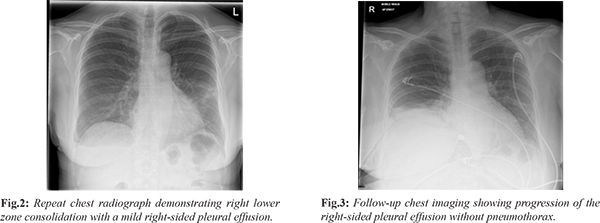
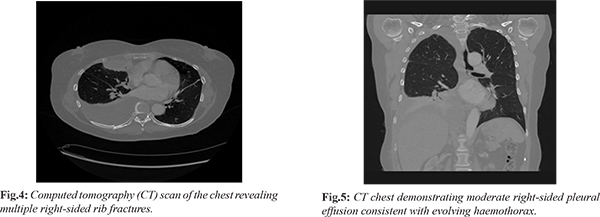
Three days later, she presented again to the Emergency Department with increasing right-sided chest pain. Clinical examination remained unremarkable. However, repeat chest radiography revealed right lower zone consolidation with a mild pleural effusion [Fig.2]. Her prior history of trauma was not adequately considered, and she was referred to the Same Day Emergency Care (SDEC) unit. A provisional diagnosis of lower respiratory tract infection was made, and she was managed with oral antibiotics and analgesics, with advice for follow-up imaging. Subsequently, the patient reported with new-onset dyspnea and persistent right-sided chest pain. On examination, reduced air entry was noted on the right side. Repeat chest imaging demonstrated a progressive increase in the right-sided pleural effusion without evidence of pneumothorax [Fig.3]. A subsequent computed tomography (CT) scan of the chest identified multiple right-sided rib fractures along with a moderate pleural effusion, suggestive of an evolving haemothorax [Fig.4,5].
The patient was transferred to the resuscitation area, where an intercostal chest tube was inserted [Fig.6], yielding approximately 1000 mL of blood. Following cardiothoracic consultation, she was admitted under the surgical team for further management. Her clinical condition improved progressively [Fig.7,8], and the chest tube was removed after seven days. She was discharged in stable condition with planned follow-up in the surgical outpatient clinic.
Discussion
Hemothorax refers to the accumulation of blood within the pleural cavity and most commonly occurs as a consequence of thoracic trauma. Both blunt and penetrating injuries can result in significant hemothorax due to laceration of the lung parenchyma, intercostal vessels, or major mediastinal structures [3,4]. In blunt trauma, the source of bleeding is frequently related to rib fractures causing injury to intercostal or intrapulmonary vessels; however, hemothorax may also develop in the absence of rib fractures or even secondary to vertebral injuries [5].
Hemothorax and hemopneumothorax are observed in approximately one-third of patients with thoracic trauma [3]. Although most cases present immediately following injury, delayed hemothorax is a recognized entity that may develop hours to days later, often with initially normal radiographic findings. The incidence of delayed hemothorax within the first two weeks has been reported to range between 7 to 12% [1,6]. This highlights the importance of careful follow-up and observation of patients discharged after blunt chest trauma, even when initial clinical and radiological assessments appear reassuring.
Clinical assessment plays a crucial role in early detection. Physical examination, particularly auscultation, has demonstrated high sensitivity (100%) and specificity (99.8%) in identifying hemopneumothorax in hemodynamically stable patients [7]. Nonetheless, imaging remains indispensable for confirmation. Chest X-ray (CXR) is typically the first-line investigation, with classical features including blunting of the costophrenic angle or hemithoracic opacity suggestive of hemothorax [2]. However, its sensitivity is limited, particularly for small or loculated collections. An erect chest radiograph may detect as little as 200-300 mL of pleural fluid, whereas in the supine position, more than 1000 mL may be required before radiographic changes become apparent [3,8,9]. In view of these limitations, computed tomography (CT) of the chest is considered the gold standard for detecting post-traumatic hemothorax and associated injuries [10]. Additionally, ultrasonography, including FAST and eFAST, serves as a valuable bedside adjunct, particularly in unstable patients or in settings where CT imaging is not readily available [11-13]. In the present case, the patient had an initially normal chest radiograph and was subsequently misdiagnosed with a lower respiratory tract infection when a small pleural effusion was identified. The diagnosis of delayed hemothorax was established only after CT imaging during her third presentation. This emphasizes the need for a high index of suspicion and a low threshold for repeat or advanced imaging in patients with persistent or worsening symptoms following blunt chest trauma.
Early recognition and prompt management, including timely drainage, are essential to prevent complications such as infection, fibrothorax, and respiratory compromise. Therefore, appropriate safety-netting advice and patient education remain integral components of management in such cases.
Conclusion
Delayed hemothorax is an important and potentially life-threatening complication of blunt chest trauma that may occur despite an initially normal chest X-ray. This case highlights the limitations of early radiographic assessment and the risk of misdiagnosis when subtle findings, such as minimal pleural effusion, are overlooked. Clinicians should maintain a high index of suspicion in patients presenting with persistent or worsening symptoms after trauma and ensure that the history of injury is carefully considered.
Appropriate safety-netting advice and close follow-up are essential for early detection. A low threshold for repeat imaging, particularly CT chest, is recommended when clinical symptoms do not correlate with initial findings. Early diagnosis and timely intervention, including chest drainage when indicated, are crucial to prevent complications and improve patient outcomes.
Contributors: MNM: Concept and participated in writing; DS: revised and approved the final manuscript; AQ: participated in writing. MNM will act as a study guarantor. All authors approved the final version of this manuscript and are responsible for all aspects of this study.
Funding: None; Competing interests: None stated.
References
- Plourde M, Émond M, Lavoie A, Guimont C, Le Sage N, Chauny JM, et al. Cohort study on the prevalence and risk factors for delayed pulmonary complications in adults following minor blunt thoracic trauma. CJEM. 2014;16(2):136-143.
- Broderick SR. Hemothorax: Etiology, diagnosis, and management. Thorac Surg Clin. 2013;23:89-96.
- Bozzay JD, Bradley MJ. Management of post-traumatic retained hemothorax. Trauma. 2019;21:14-20.
- Boersma WG, Stigt JA, Smit HJ. Treatment of haemothorax. Respir Med. 2010;104:1583-1587.
- Yu H, Isaacson AJ, Burke CT. Management of traumatic hemothorax, Retained hemothorax, and other thoracic collections. Curr Trauma Rep. 2017;3:181-189.
- Misthos P, Kakaris S, Sepsas E, Athanassiadi K, Skottis I. A prospective analysis of occult pneumothorax, delayed pneumothorax and delayed hemothorax after minor blunt thoracic trauma. Eur J Cardiothorac Surg. 2004;25:859-864.
- Bokhari F, Brakenridge S, Nagy K, Roberts R, Smith R, Joseph K, et al. Prospective evaluation of the sensitivity of physical examination in chest trauma. J Trauma Inj Infect Crit Care. 2002;53:1135-1138.
- Demetriades D, Talving P, Inaba K. Chest trauma. In: Oestern H-J, Trentz OL, Uranues S, eds. Head, Thoracic, Abdominal, and Vascular Injuries. Berlin, Heidelberg: Springer Berlin Heidelberg; 2011:223-255.
- Feden JP. Closed Lung Trauma. Clin Sports Med. 2013;32:255-265.
- Trupka A, Kierse R, Waydhas C, Kolb DN, Blahs U, Schweiberer L, et al. Shock room diagnosis in polytrauma. Value of thoracic CT. Unfallchirurg. 1997;100:469-476.
- Chung MH, Hsiao CY, Nian NS, Chen YC, Wang CY, Wen YS, et al. The Benefit of ultrasound in deciding between tube thoracostomy and observative management in hemothorax resulting from blunt chest trauma. World J Surg. 2018;42:2054-2060.
- Staub LJ, Biscaro RRM, Kaszubowski E, Maurici R. Chest ultrasonography for the emergency diagnosis of traumatic pneumothorax and haemothorax: A systematic review and meta-Analysis. Injury. 2018;49:457-466.
- Mowery NT, Gunter OL, Collier BR, Haut E, Diaz JJ, Hildreth A et al. Practice management guidelines for management of hemothorax and occult pneumothorax. J Trauma. 2011;70:510-518.